




Imaging of Spinal Stenosis

The incidence of spinal stenosis is on the rise in the general population. As the population continues to age and the average life span increases, spinal stenosis will become an even more prevalent cause of lower back pain. Degenerative causes remain the predominant factor in the development of spinal stenosis. Less likely are congenital causes, as well as developmental and pathologic causes. This article will focus on the degenerative changes commonly precipitating lumbar spinal stenosis.
Older patients in whom spinal stenosis is suspected should be examined initially, using conventional spinal radiographic imaging. Cervical stenosis assessment in older patients should include anteroposterior (AP), lateral, oblique, and swimmer’s lateral views. Assessment of the lumbar spine should include a lower lumbar centered, AP, lateral, and oblique projections. Lateral views are most sensitive for central spinal stenosis, whereas oblique views of the cervical and lumbar areas better demonstrate lateral stenosis syndromes. In older patients, radiography of the cervical, thoracic, and lumbar spine have value for screening for compression fractures or spondylosis. If the patient is symptomatic with radiculopathy, weakness or altered gate, MRI of the spine is the preferred method. CT of the spine should be limited to trauma and to those patients who have contraindications for MRI. MRI provides the best quantitative analysis of stenosis and demonstrates soft tissue components that cannot be seen on plain film, such and disc bulging, ligamentum flavum hypertrophy and synovial cysts.
Advertisement

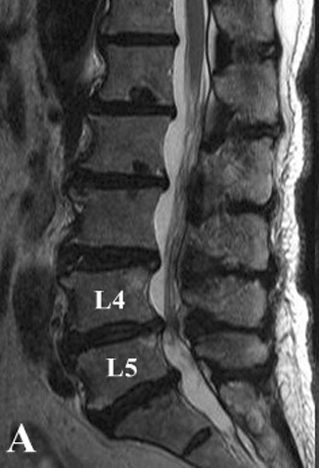
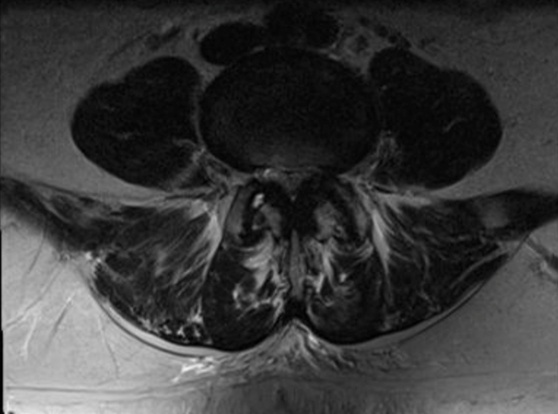
Central canal stenosis in the lumbar spine due to degenerative causes may include any of the following findings on MRI: disc bulging, ligamentum flavum hypertrophy, facet hypertrophy or synovial cyst. All may result in some degree of compromise of the central canal, and, when present in combination, can drastically alter the size of the canal. Figures 1 and 2 demonstrate diffuse degenerative disc bulging and ligamentum flavum hypertrophy, with the resultant marked decrease in the volume of the central canal and impingement of the thecal sac.
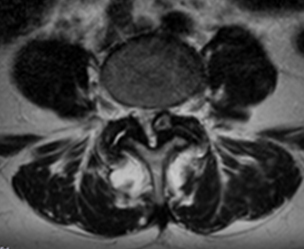
Synovial cysts emanate from the facet joint and are deep to the ligamentum flavum and facet joint capsule. They may protrude into the central canal. Figure 3 features a left-sided synovial cyst with facet hypertrophy and severe encroachment of the central canal.
Facet arthrosis features a decrease in facet joint spacing to various degrees and can result in an anterolisthesis of one vertebra on another. This is referred to as a “degenerative spondylolisthesis.” Encroachment of the central canal and intervertebral foramen may result.
A subtype of central canal stenosis is lateral recess stenosis. The lateral recess is bounded anatomically by the vertebral body, pedicle, and facet. With facet hypertrophy, this space may be compromised and nerve roots may become entrapped.
The cervical spine is unique, in that there is an addition to the osseous anatomy of the vertebral body. This consists of the uncinate processes. When there is proliferation of the uncinates, they may encroach upon the intervertebral foramen and produce foraminal stenosis. In addition, degenerative spondylolistheses may occur in the cervical spine due to facet arthrosis, which may further encroach upon the IVF.
As a guide to ordering MRI for the purpose of evaluating spinal stenosis, I offer the following information:
- MRI examinations for the purpose of evaluating spinal stenosis do not usually need to be performed with intravenous contrast. One caveat is if there is a history of prior disc surgery, particularly if recent. In this case, contrast may be of benefit.
- A fat suppressed sequence is always helpful in any MRI examination, and most imaging facilities will include one in their routine spinal scan.
- Axial and sagittal imaging planes are typically utilized; however, there may be a coronal sequence included as well.
- Axial sequences are routinely provided with T-1 and T-2 weighting in the lumbar spine and T-1 and gradient echo weighting in the cervical spine.
Spinal stenosis is well seen on MRI. If plain films are suggestive of stenosis, an MRI examination will help quantify the degree of stenosis and aid in prognosis and evaluating treatment options.
filings.









{kind=link}