




MRI Detection of Paraspinal Muscle Atrophy in Lower Back Pain

In the United States, lower back pain (LBP) is the second most common reason for a patient to consult a doctor, surpassed only by upper respiratory infections (1). LBP is also one of the leading causes of disability during one’s working years (2) (3). Within the past several years, there has been increasing attention paid to the concept of decreased paraspinal muscle mass/fatty replacement and its relation to the development and persistence of LBP. There has been speculation about the significance of this finding and whether the atrophy is due to the LBP or, conversely, the LBP is due to the atrophy.
MRI
An interesting facet of this discussion has been the ability of MRI to non-invasively quantify paraspinal muscle atrophy and identify the fatty replacement. Because strengthening of the lumbar muscles is a commonly recommended adjunct to spinal manipulation in the treatment of LBP, it may be important to clarify whether lumbar muscle atrophy has a relationship to LBP. Fat infiltration seems to be a later stage of muscular degeneration, and can be measured using magnetic resonance imaging. Specifically, fatty atrophy of the multifidus muscle group has been linked in a number of studies with an increased incidence of lower back pain (4) (5). This has been largely correlated with chronic lower back pain, although some studies also suggest that there may be a link in acute LBP as well [A]. It is generally believed that muscular insufficiency and LBP are linked, even though the main direction of this link is unclear. Is LBP caused by insufficient muscular strength or control, or does LBP affect the muscles and their function?
Advertisement
Atrophy of paraspinal muscles is common in LBP (15A). It has been estimated that atrophy of the paraspinal muscles occurs in 20%-60% of people suffering with chronic lower back pain. Specifically, a decreased cross-sectional volume of the multifidi at the L4 or L5 levels has been reported to be associated with LBP pain in the recent literature (17A). Histologically there are changes in muscle fiber type that are not perceptible on MR imaging. Paraspinal muscle atrophy in chronic LBP is associated with variable changes in muscle fibers, including reduced type I and II muscle fiber size, decreased type II muscle fiber cross-sectional area, no change in muscle fiber size, and increased core targetoid and moth-eaten muscle fibers [B]. Overall, the muscle atrophy tends to be more diffuse in chronic LBP, and, thus, it is surmised that it may be related to deconditioning or disuse.
There has been reported change in the multifidus cross-section area only 24 hours post-acute lower back pain episode. However, the latency and mechanism for these rapid changes remain controversial. Initial studies reported no change in muscle obtained during surgery for acute LBP. Other data point to fatty replacement of muscle, which is common in other muscle disorders. Disuse and denervation have been postulated as explanations for muscle atrophy in cases of acute LBP. However, disuse is expected to have a generalized effect, and this mechanism is thought to be less likely. In cases of disc herniation and neural compression, signs of paraspinal denervation and reinnervation are common. Moreover, localized changes in histochemistry have been reported in muscle fibers from a single lumbar segment.
MR Spectroscopy
Based on the understanding of the scientific literature in this area, it is hypothesized that acute LBP leads to altered neuromuscular functioning, which, in turn, results in changes in muscle histology, seen as atrophy. However, the cross-sectional area of the muscle may not decrease, due to fatty infiltration in the muscle bundle. Fat infiltration can be seen on magnetic resonance imaging (MRI) and in human cadaver studies. Unaided MRI has been shown to be a valid method of identifying muscle volume and the amount of fat in human skeletal muscle but is not particularly sensitive to early fat infiltrative changes. These changes have been shown to occur; however, a more sensitive modality is required to detect them. MR spectroscopy has shown changes in muscle that did not demonstrate change on MR alone (A).
Assessment of paraspinal muscle volume may be worthwhile to include on a lumbar spine MRI report. From a clinical perspective, this finding may be of use in substantiating LBP and the need for treatment. There are several grading scales used for quantification of fatty paraspinal muscle atrophy. One system utilizes the presence of fatty infiltration within muscle. Fat infiltration of the muscle was visually graded using the standard criteria: “normal” for estimates of 0–10% fat within the muscle, “slight” for 10–50% fat, and “severe” for >50% fat. An alternative grading system utilizes assessment of total muscle volume, which allows more precise quantification with grading ranging from 1-4 [C]. Grade (1) is a decrease in volume up to and including 24%, grade (2) 25-49%, grade (3) 50-74% and grade (4) 75-100%. Grade assessment is made at the L5 level.
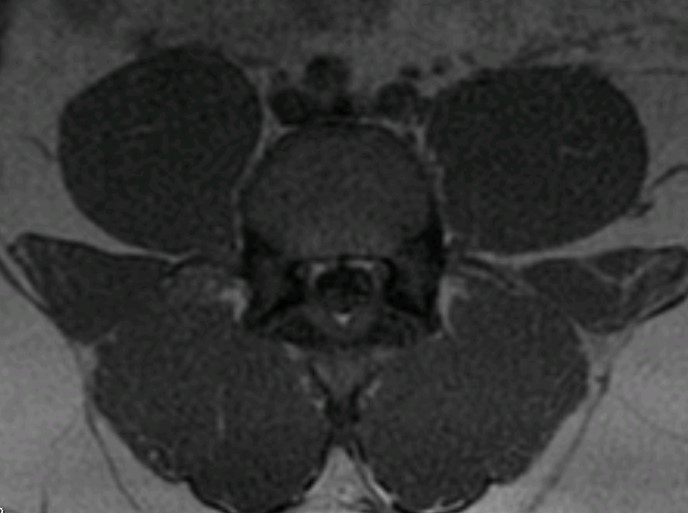
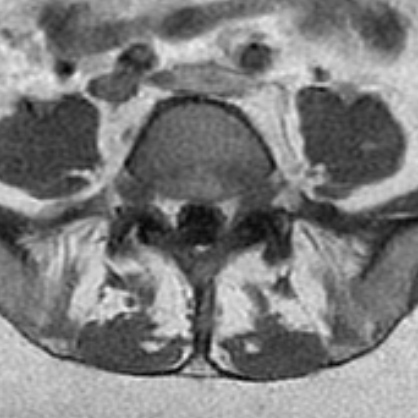
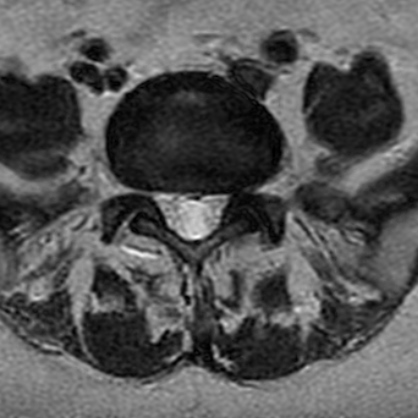
Figure 1 is a T-1 axial image demonstrating normal, well-developed paraspinal musculature. Contrast this with figure 2, a T-1 weighted axial image that displays marked paraspinal muscle atrophy. Figure 3 is a T-2 weighted axial image of the same patient as figure 2. On the scale assessing total muscle volume, this degree of atrophy is rated as 3, between 50 and 74% of volume loss.
Conclusion
To recap, fatty atrophy of paraspinal musculature may be linked to an increased incidence of chronic LBP and possibly acute LBP as well. MRI is well suited to demonstrate quantitatively paraspinal muscle volume loss. Demonstration of loss of paraspinal muscle volume may help to substantiate LBP and the need for treatment.
References:
- Per Kjaer, Toam Bendix, Joan Salgaard Sorenson, Lars Karsholm, Charlotte Lebaeuf-Yale, “Are MRI-defined Fat Infiltrations in the Multifidus Muscle Associated with Low Back Pain?” BMC Medicine 2007, 5: 2 doi; 10, 1186/1741-7015-2
- Paul Hodges, PhD; Allison Kaible Holm, PhD; Tammy Hanson, PhD; Stan Holm, PhD, “Rapid Atrophy of the Lumbar Multifidus Follows Experimental Disc or Nerve Root Injury”, Spine 2006;31(25): 2926-2933
- Mark L. Prasarn, Vasalos Kostantinos, Ellen Coyne, John Wright, Glenn R. Rechtine,
“ Does lumbar paraspinal muscle fatty degeneration correlate with aerobic index and Oswestry disability index?” Surg Neurol Int. v. 6





{kind=link}