




Diffuse Idiopathic Skeletal Hyperostosis (DISH): A Common Yet Complicated Condition

Diffuse idiopathic skeletal hyperostosis (DISH) is not an uncommonly encountered condition for the chiropractic physician. It is estimated that up to 10% of older individuals are affected, typically beginning in the 5th and 6th decades (1). It is important to remember that DISH has an association with diabetes mellitus, obesity, and metabolic syndrome (1). As the incidence of those conditions rise, so does the incidence of DISH.
DISH is characterized by flowing hyperostosis of the anterior longitudinal ligament, involving at least four continuous vertebral levels. Enthesopathy at the site of tendinous and ligamentous attachments, especially about the pelvis, is also characteristic. DISH is most common in the thoracic spine, but also occurs in the cervical and lumbar spine. Intervertebral disc heights tend to be maintained due to the “scaffolding” effect provided by the ossification anteriorly. Clinically, DISH tends to be either asymptomatic or present as spinal stiffness. However, there are several associated conditions and risk factors that should be considered and assessed in your patients with DISH, as some can have serious clinical consequences. Some of the associated conditions and risk factors include: 1) Ossification of the posterior longitudinal ligament; 2) chalk stick fracture; and 3) dysphagia.
Advertisement
1) Ossification of the posterior longitudinal ligament (OPLL)

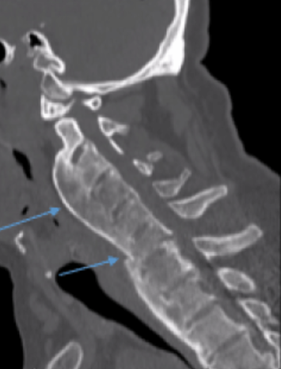
OPLL is present in approximately 50% of patients with cervical DISH and is most common in the cervical spine, representing 75% of all OPLL cases (2). OPLL may occur in the thoracic and lumbar spine as well. It is twice as common in men than women and slightly more common in Asian countries (3). Patients with OPLL may be asymptomatic or present with symptoms consistent with central canal stenosism such as radiculopathy and myelopathy. Cord injury from minor trauma is also a greater risk in those patients with OPLL, particularly in the cervical spine. CT imaging is the best imaging modality to assess the degree of central canal stenosis. Treatment may be conservative, but surgical treatment may be appropriate when neurologic symptoms are present. Great care and caution should be taken when assessing and treating your patients with OPLL.
2) Chalk stick fracture
The most important risk fracture of DISH with or without OPLL is the risk of a chalk stick fracture due to ankylosis of the spine. Most all practitioners easily remember the risk of chalk stick (aka carrot stick) fracture in inflammatory spondyloarthropathies such as ankylosing spondylitis, but often fail to recognize DISH as a risk factor for this same type of fracture. A chalk stick fracture is an unstable fracture through ankylosed vertebrae, regardless of the etiology of the ankylosis. These fractures can occur following minor trauma, such a trip on a curb, in conditions such as AS and DISH.
A systemic review of the literature in 2009 by The European Spine Journal analyzed outcomes in patients with AS and DISH with cervical spinal fracture resulting from low energy injury. This review found that 67% of patients with AS and 40% of patients with DISH had neurologic deficits. More strikingly, though, the study found that the incidence of mortality at three months post trauma was 20% in patients with DISH and 17% in patients with AS (4).
It is important to remember that high velocity low amplitude chiropractic manipulation is contraindicated in ankylosis of the spine, no matter the etiology. DISH is a common cause of vertebral ankylosis, and therefore HVLA manipulation would be contraindicated in those patients that have DISH with osseous ankylosis across vertebral levels.
3) Dysphagia

Bulky hyperostosis the anterior longitudinal ligament in the cervical spine can result in posterior compression of the esophagus. Resection of the bulky hyperostosis in the region may be needed to relieve the mechanical symptoms.
Conclusion
In conclusion, DISH is a commonly encountered condition that is often incidentally noted on radiographs in otherwise asymptomatic patients. But it is important for the clinician to understand the potential associated conditions, as well as the potentially catastrophic risk factors, such as osseous ankylosis, that may be present in some patients with DISH.
References:
1) Kuperus J, Mohamed Hoesein F, de Jong P, Verlaan J. Diffuse Idiopathic Skeletal Hyperostosis: Etiology and Clinical Relevance. Best Practice & Research Clinical Rheumatology. 2020;34(3):101527.
2) Nguyen T, Yahara Y, Yasuda T et al. Morphological Characteristics of DISH in Patients with OPLL and Its Association with High-Sensitivity CRP: Inflammatory DISH. Rheumatology (Oxford). 2022;61(10):3981-8.
3) Saetia K, Cho D, Lee S et-al. Ossification of the posterior longitudinal ligament: a review. Neurosurg Focus. 2011;30 (3)
4) Westerveld, L.A., Verlaan, J.J. & Oner, F.C. Spinal fractures in patients with ankylosing spinal disorders: a systematic review of the literature on treatment, neurological status and complications. Eur Spine J 18, 145–156 (2009).
5) Singh S (2018) Chalk stick break. Rheumatol Orthop Med: doi: 10.15761/ROM.1000158










{kind=link}