




Whiplash
Common Whiplash Symptoms
Many articles that have been written were presented primarily for those practitioners who have never treated patients injured in Motor Vehicular Crashes (MVC), whether recent graduates or seasoned DCs. They have also been presented only as a refresher for those who are very familiar with these injuries resulting from MVC. This article will deal with symptoms associated with “Whiplash” or for those who know it as “Cervical Acceleration/Deceleration Disorder,” or CAD trauma.
The symptoms most commonly described following CAD injury are described in their general order of prevalence. This is not, however, a thorough list.
Advertisement
Acute and subacute CAD symptoms
- Neck pain (92%)
- Headache (57%)
- Interscapular pain (42%)
- Back pain (39%)
- Paresthesia (30%)
- Extremity pain/weakness (6% – 12%)
- Cognitive difficulties (26%)
- Dizziness/light-headedness (15%)
- Facial pain and TMJ related symptoms (clicking; closed lock; etc.) 4%+
- Auditory symptoms (phonophobia; tinnitus; loss of hearing)
- Vertigo (4%)
- Ocular dysfunction (blurred vision; photophobia) (21%)
Let us now review the following with possible indications of cause.
Neck pain
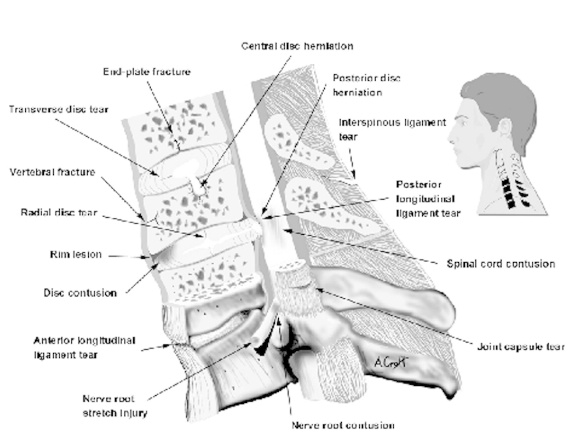
Tearing or damage to any soft tissue (including nervous tissue), fracture of bone, or disc herniation/ prolapse/protrusion/disruption can cause neck pain.
This is an illustration of part of the cervical spine (black portion of inset). Part is cut in half for better viewing. This illustrates all of the lesions that have been reported to occur in whiplash trauma. With permission from Whiplash! A Patient’s Guide to Recovery. San Diego, (c) Spine Research Institute of San Diego, 1999.
Neck stiffness
- Stiffness may be the result of protective muscle spasm secondary to most injuries of the neck.
- Chronic stiffness indicates myofascial fibrosis or contraction, ligamentous contraction (particularly of joint capsules), disc degeneration, or secondary osteoarthritic change.
Shoulder pain (53%)
- This can be either from direct injury to the shoulder, such as from a shoulder harness, or impact with the car’s interior, or from referred pain from soft tissues of the neck or a disc lesion.
- Other causes of shoulder pain, such as impingement syndrome, thoracic outlet syndrome (TOS), and rotator cuff inflammation, may develop secondary to CAD trauma
Headaches
These are the result of either injury to the upper cervical spine, or reflex or protective muscle spasm in the neck. One cannot ignore Post Concussion Syndrome/Post Traumatic Headache as a result of Mild Traumatic Brain Injury (MTBI) where cognitive difficulties are noted, as well as dizziness and lightheadedness.
Intrascapular pain
- This pain is caused either by direct injury to paraspinal muscles or, more commonly, as a result of referred (scleratogenous) pain from the neck.
- It also may be seen with disc lesions.
As ICS mentor in PI cases, I had received numerous calls regarding low back pain and MVC. With the comprehension of the biomechanical changes that occur to the occupants of the vehicle in MVC has assisted those in understanding low back injuries. The following had been noted in various studies:
Back pain
- Croft and Foreman found low back pain (LBP) in 57% of their CAD cases (71% in broadside collisions).
- Braaf and Rosner found LBP in 42% of their cases.
- Hohl found LBP in 35% of his cases.
- Twenty-five percent of the patients in Hildingsson and Toolanen’s study had low back pain.
- In a recent study of chiropractic therapy in CAD patients, it was found that patients with low back pain generally required more treatment than those with neck pain alone.
- In a prospective study, Gargan and Bannister reported 32% of their group as having LBP and an additional 10% developed LBP as a late manifestation.
- This same percentage (32%) was found by Bring and Westman. Magnússon reported an incidence of 48% with LBP.
The exact mechanism of low back injury in rear impact collisions, although not entirely clear, is in all probability multifactorial. Factors affecting the incidence, nature, and severity of low back injury in automobile crashes include the following:
- Position of the occupant in vehicle,
- The use or non-use of seat belts and shoulder harness,
- Deployment of airbag system, (which are designed to deploy only with frontal impacts, but may deploy in more severe secondary collisions),
- Type of restraint system (i.e., conventional restraints vs. restraints with pretensioners),
- Stiffness of the seat back,
- Inclination of the seat back,
- Properties of the seat back padding,
- Degree of ramping,
- Vector and severity of the collision,
- Second collisions inside or outside the occupant’s vehicle,
- Snugness of the restraint system,
- Positioning of the restraint system on the occupant,
- Positioning of the restraint system anchors within the vehicle,
- Physical makeup of the occupant, including stature, build, age, and level of fitness, and
- Preparedness for the collision.
With the knowledge of what was provided will further enable the practitioner in providing appropriate care. But, prior to providing the care that is needed, it all relates to taking a proper history and performing a thorough examination.
Bibliography:
Foreman SM, Croft AC: Whiplash Injuries: The Cervical Acceleration/Deceleration Syndrome.Baltimore, Williams & Wilkins Co., 1999










