




5 Solutions for Peripheral Pain

Chronic pain is an outward manifestation of inner adaptations to pain processing. The brain is responsible for pain perception and remembering pain patterns. However, in addition to the brain, the dorsal horn of the spinal cord and peripheral tissue can also LEARN to be in pain.
Learning is a physiologic process and not an intellectual feat, and it doesn’t happen only in the brain. Each site adapts physiologically in response to constant stimulation. This blog will highlight five evidence-based treatment concepts to help stop peripheral nociception, the instigator of chronic pain.
Advertisement

Peripheral Learning
Pain is an unpleasant sensation usually evoked by the activation of nociceptors in response to harmful high-intensity stimuli. What distinguishes the nociceptive system from other perceptual systems is its responsiveness to repeated stimuli.
In the case of innocuous stimuli, repetition typically reduces the response, a phenomenon referred to as HABITUATION. In contrast, repetition of a noxious stimulus can induce a progressive amplification of the usual response to the stimulus, i.e.,SENSITIZATION. The nociceptive system tends to increase its responsiveness when exposed to repeated stimulation.
Habituation and sensitization are two necessary forms of non-associative learning. Habituation would generally allow a person to filter out irrelevant sensory input about their environment whereas sensitization would increase the ability to respond to stimuli, potentially compromising the integrity of the organism and survival, thus fulfilling a protective role. (1)
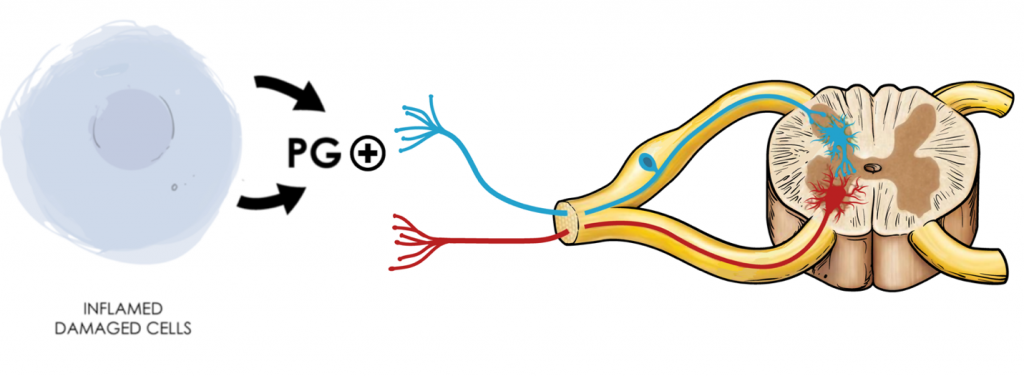
Fig 1. Pain perception begins with peripheral tissue irritation from a mechanical insult, heat, or chemical irritation. The affected tissue and surrounding immune cells start releasing pro-inflammatory cytokines like prostaglandins. Sensory nerve fibers (1st order neurons) will respond to prostaglandin stimulation and carry the signal or impulse to the spinal cord’s dorsal horn
Solution 1: Manual Therapy
Pain from ongoing musculoskeletal pathology produces continual nociceptive input. Reducing peripheral pain utilizing manual therapy may prevent centralization of symptoms. (2) Select the right treatment for the right patient. The ability to reduce tension and mobilize joints is paramount to the restoration of musculoskeletal function.
Solution 2: Spinal Manipulation
Chronic nonspecific LBP patients treated with spinal manipulation experience local and remote hypoalgesia, along with improved pain and disability. (3) Spinal manipulation provides short-term analgesia and long-term pain reduction when supplemented with the appropriate rehab or ADL modification.
Solution 3: Diet
Metabolic interventions, such as low-carbohydrate or ketogenic diets, are promising new avenues for diminishing hyperexcitability of the CNS in chronic pain patients. (4) Changing someone’s diet is difficult since eating is habitual. If you don’t possess the time or knowledge to address dietary contributors, find someone in your area who does.
Basic Nutrition Advice
Solution 4: BMI
One molecular hallmark of caloric excess and obesity is chronic inflammation, particularly in visceral adipose tissue (VAT). Over time, obese VAT becomes increasingly populated by pro-inflammatory cells, and the proportion of anti-inflammatory regulatory cells declines. (5) Increasing your patient’s activity level has multiple benefits. Exercise will increase the descending inhibitory pathway while promoting healthy habits, leading to weight loss.
Solution 5: Sleep
Among people with chronic pain, insomnia is highly prevalent, closely related to the mechanism of chronic pain, and characterized by low-grade neuroinflammation. (6) Consultation with a sleep specialist may help you and your patients understand the underlying mechanisms behind their insomnia. Remember, pain at night is a red flag and warrants further workup. However, pain limiting the ability to fall asleep may indicate chronic pain from psychological or musculoskeletal etiologies. (7)
Tips for Healthy Sleep
If we are to accept the immense privilege of helping people understand their pain and how they can recover from it, then we are absolutely obliged to know what it is we are talking about and if that requires some serious work, then so be it. -Mick Thacker
Commentary
Traditional management of peripheral pain syndromes involves a combination of interventions, depending on the treating healthcare professional. The conventional model of biomechanical pain assumes that there is a direct linear link between the amount of structural damage and the pain experienced by the patient. According to this model, addressing the underlying pathology should result in a reduction or (complete) resolution of symptoms and subsequent recovery of normal function. However, chronic pain does not always adhere to this biomedical model of pain, as repeated stimulation may result in sensitization of peripheral and central neural circuitry. Thus, it is common to observe a discordance between the degree of structural damage and the number of symptoms experienced by the patient.
References
- Filbrich L, van den Broeke EN, Legrain V, Mouraux A. The focus of spatial attention during the induction of central sensitization can modulate the subsequent development of secondary hyperalgesia. Cortex. 2020 Mar 1;124:193-203.
- Lluch Girbés, E., Meeus, M., Baert, I., & Nijs, J. (2015). Balancing “hands-on” with “hands-off” physical therapy interventions for the treatment of central sensitization pain in osteoarthritis. Manual Therapy, 20(2), 349–352. doi:10.1016/j.math.2014.07.017
- Bond BM, Kinslow CD, Yoder AW, Liu W. Effect of spinal manipulative therapy on mechanical pain sensitivity in patients with chronic nonspecific low back pain: a pilot randomized, controlled trial. Journal of Manual & Manipulative Therapy. 2020 Jan 1;28(1):15-27.
- Koh IJ, Kang BM, Kim MS, Choi KY, Sohn S, In Y. How Does Preoperative Central Sensitization Affect Quality of Life Following Total Knee Arthroplasty?. The Journal of Arthroplasty. 2020 Apr 10.
- Stubbs, B. J., & Newman, J. C. (2020). Ketogenic diet and adipose tissue inflammation—a simple story? Fat chance! Nature Metabolism. doi:10.1038/s42255-019-0164-2
- Nijs J, Malfliet A, Ickmans K, Baert I, Meeus M. Treatment of central sensitization in patients with ‘unexplained’chronic pain: an update. Expert opinion on pharmacotherapy. 2014 Aug 1;15(12):1671-83.
- Nijs J, Mairesse O, Neu D, Leysen L, Danneels L, Cagnie B, Meeus M, Moens M, Ickmans K, Goubert D. Sleep disturbances in chronic pain: neurobiology, assessment, and treatment in physical therapist practice. Physical therapy. 2018 May 1;98(5):325-35.
- Ueberall, M. A., Essner, U., Mueller-Schwefe, G. H. (2019). Effectiveness and Tolerability of THC:CBD Oromucosal Spray as Add-On Measure in Patients With Severe Chronic Pain: Analysis of 12-Week Open-Label Real-World Data Provided by the German Pain E-Registry. J. Pain Res. 12, 1577–1604. doi: 10.2147/JPR.S192174
- Gulbransen, G., Xu, W., Arroll, B. (2020). Cannabidiol Prescription in Clinical Practice: an Audit on the First 400 Patients in New Zealand. BJGP Open. doi: 10.3399/Bjgpopen20x101010










{kind=link}