

The importance of CNS integrity and function is a central premise among most chiropractic physicians and in which much of our treatment is based. Whether it is a disc pathology or a peripheral entrapment in the extremities, it is safe to say that most all of us are confident and arguably the most competent healthcare professionals in treating these types of lesions.
Anatomy
However, when it comes to lesions above the spine, many of us may not feel as confident in the diagnosis or treatment. Not because we were not trained in the diagnosis of virtually every ailment, but because we don’t have the opportunity to see it in practice every day. So it is with this article I hope to refresh your memory of the visual pathway, and how to locate where the lesion is located if a patient were to walk into your office with a headache and loss in a visual field.
Advertisement

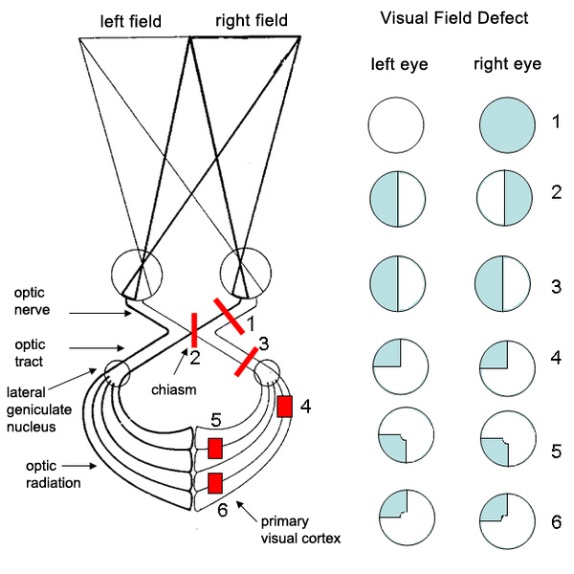
I will begin with a review of anatomy (see Fig. 1). Vision begins at the photoreceptors in the retinal layer of cells at the back of the eye. This input is then transmitted via the optic nerve into the brain to the optic Chiasm. Beyond the Chiasm, the axons are called the optic tract that wraps around the midbrain to synapse in the lateral geniculate nucleus. From here axons fan out as the optic radiations that travel through the temporal (Meyer’s loop) and parietal lobes to the back of the brain and primary visual cortex.
Remember that visual images as they pass through the lens and project onto the retina are inverted (flipped vertically and horizontally). Therefore, the temporal retina of the right eye and the nasal retina of the left eye see the left half of the world while the temporal retina of the left eye and the nasal retina of the right eye see the right half of the world.
Lesions:
1. A pattern demonstrating damage at the right optic nerve and results in complete loss of vision in the right eye. This may be seen if the patient had an optic nerve glioma anterior to the chiasm.
2. A pattern where the lesion at the optic chiasm disrupts the axons from the nasal field of both eyes resulting in the loss of vision of the right half of the right visual field and the left half of the left visual field. This visual defect is called non-homonymous bitemporal hemianopia. A non-homonymous deficit refers to different halves of the visual field in each eye. This is frequently caused by a pituitary adenoma compressing the optic chiasm. This may be accompanied by amenorrhea in women and reduced sperm count in men. Pituitary tumors may also secrete prolactin and growth hormone.
3. A lesion of the right optic tract that carries axons from the ganglion cells of the temporal retina of the right eye and the nasal retina of the left eye (both see objects in the left visual hemifield) result in blindness in the left field of vision. This visual disorder is called contralateral left homonymous hemianopia. A homonymous deficit refers to the same half of the visual field of each eye. The visual deficit in this lesion would be the same if it involved the whole optic radiation just distal to the LGN (Lateral geniculate nucleus).
4. A lesion to the right temporal lobe (Meyer’s loop) carries visual information projected from the left superior visual hemifield of each eye. This order is referred to as a superior left homonymous quadrantanopia (pie in the sky disorder). This type of deficit may be seen when a patient has experienced a vascular injury to the middle cerebral artery.
5. A lesion in the right parietal lobe carries information projected from the left lower visual hemifield of each eye. This order is referred to as an inferior left homonymous quadrantanopia (pie on the floor disorder). This type of deficit may be seen when a patient has experienced a vascular occlusion of the middle cerebral artery.
Conclusion
When trying to locate lesions in the visual pathway, it helps to recall that images are inverted (both vertically and horizontally) when they enter the eye. Objects from the left visual field are projected to the right visual cortex and objects from the right visual field to the left visual cortex. Also, objects in the superior visual fields are projected through the lower temporal lobe and objects from the lower visual fields are projected through the parietal lobe.
References:
1. Cerebral Arterial Territories with Watershed Areas. Retrieved July 5, 2013, from http://missinglink.ucsf.edu/lm/ids_104_cns_injury/response%20_to_injury/watershed.htm
2. Basic Visual Pathway. Retrieved July 8, 2013, from http://www.bioon.com/bioline/neurosci/course/basvis.html
3. Raed Behbehani, M.D., FRCSc. Anatomy and Lesions of Visual Pathways. Retrieved July 8, 2013, from http://www.slideshare.net/neurophq8/anatomy-and-lesions-of-visual-pathways
4. Fig 1. Reference







