




The Overhead Athlete from Pain to Performance

Recently, I was asked to do a webinar for the ACA (American Chiropractic Association) on the UE (upper extremity). Upper extremity injuries and the throwing athlete are topics about which I’m well versed and passionate. It’s an area that I’m happy to humbly share what I know and admit what I don’t know. The model I used was taking the patient from pain and transitioning him or her into the realm of performance. I’d like to share some of what was discussed in the 2-part webinar, “The Overhead Athlete from Pain to Performance.” Please keep in mind that the webinar serves as a bridge into a 12-hour seminar that has lecture and lab components. The info below is an overview of the material.
Specialization in Sports and Increased Injury Risk
The term “overhead athlete” means, of course, an athlete that uses repetitive movements of the arm overhead, placing greater than normal stress on the involved joints and connective tissue. The explosion of specialization in youth sports shows increased incidence of shoulder and elbow injuries. Clinical reports by famed orthopedic surgeon James Andrews indicate that he’s seen a 10-fold increase in “Tommy John surgeries” (UCL – ulnar collateral ligament reconstruction) since 2000. (1) This scenario is being repeated for other UE injuries in the young overhead athlete.
Advertisement

Nasty UCL Surgical Scar
The Overhead Throwing Motion
Overhead athlete mechanics are a whole kinetic chain event. Learning how to assess and treat the kinetic chain is critical in this population. A good first step is understanding the how parts should work in isolation and then integrating that into your understanding of the kinetic chain. Some critical areas include the shoulder and elbow.
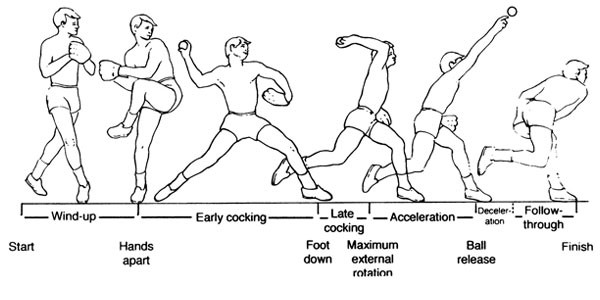
The throwing motion is a whole kinetic chain event
Anatomy and Biomechanics
The shoulder (GH-Glenohumeral) joint is not a true ball and socket. It is more like a ball and saucer. This configuration means the joint has great mobility at the expense of stability. Great amounts of neuromuscular control for support and stability is required. If the neuromuscular control isn’t sufficient, great stress is placed on the passive shoulder structures, such as the labrum, capsule, articular cartilage, and the glenohumeral ligaments.

A good analogy for the ball and saucer configuration of the GH Joint
Preserving the subacromial space is critical in the overhead athlete. The subacromial space has some key structures, such as the long head of the biceps tendon, superior GH capsule, supraspinatus tendon, upper part of the infraspinatus, upper portion of the subscapularis, subacromial bursa and the inferior surface of the AC (acromioclavicular) joint that pass through it.
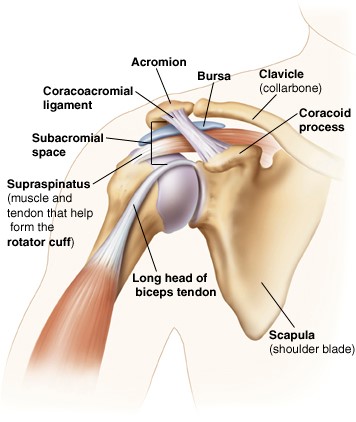
Subacromial space anatomy
Force couples are critical in the shoulder to preserve the subacromial space. Namely, the rotator cuff muscles and the deltoid, as well as the internal vs. external rotators, work to maintain normal articulation and center of rotation (“centration”) of the joint. These force couples in an ideal situation provide synergistic compression and distraction of the joint. The byproduct of these strategies is commonly referred to as “reflexive stabilization.”
Centration, Stabilization, Subacromial Impingement & The Painful Arc
When the joint is not “centrated” and when “reflexive stabilization” is not functioning properly, a painful arc may develop. A painful arc is created when the athlete experiences pain with elevation, namely abduction, in the range of 60-120 degrees. Painful arc syndrome is just one consequence of the loss of both “centration” and “reflexive stabilization.” Painful arc syndrome is indicative of rotator cuff pathology or subacromial impingement. A painful arc and subacromial impingement are signs rather than true diagnoses. Those signs require a bit more investigation.
What Does the Rotator Cuff Really Do?
This brings up the question: what does the rotator cuff do? Many of us were taught in our anatomy courses that the rotator cuff performs internal and external rotation. That’s partially correct. The rotator cuff provides more to the shoulder than just motion. The cuff additionally provides 1) centration and reflexive stabilization; and 2) eccentric control.
The cuff promotes centration and reflexive stabilization by providing resistance against compression and distraction forces Eccentric control leads to deceleration of the UE during overhead motions (example: the pitching motion). It is important to remember that when we structure a compressive rehab program for the overhead athlete that we include components that challenge centration, reflexive stabilization and eccentric control functions of the shoulder.
The rotator cuff does this (external rotation and internal rotation range of motion)

AND THIS (Anti-compression)
AND this (anti-traction)
Glenohumeral Internal Rotation Deficit & Total Arc Range of Motion Deficit
Internal rotation and total arc range of motion are critical in the overhead athlete. GIRD (Glenohumeral Internal Rotation Deficit) is characterized by decreased dominant side internal rotation vs. the non-dominant side (2,3). The deficit is characterized as functional or adaptive if it is less than 18-20 degrees from the dominant to the non-dominant arm. The deficit is considered pathological if it exceeds 20 degrees.
Pathological GIRD may lead to capsular restriction, muscle stiffness, humeral retrotorsion and other compensatory degenerative changes in the shoulder. Humeral retrotorsion is shifting of the humeral head posteriorly as an adaptive response to the stress placed on the GH joint by the overhead athlete. The implication of this finding, humeral retrotorsion, is unclear (4). It is theorized that humeral retrotorsion is an adaptive response to stress with the potential for protective value; however, humeral retrotorsion also could theoretically predispose the overhead athlete to conditions such as internal impingement of the shoulder or posterior superior labral pathology.
A newer model incorporates the concept called “total arc range of motion.” This model looks at dominant vs. non-dominant arm internal and external range of motion. If the combined amounts of internal + external rotation show a 5 degree or more side to side deficit, research suggests a 2.5-2.6x increased likelihood of a shoulder or elbow injury respectively in a throwing athlete, compared to those without such a deficit (2, 5,6,7).
A daily stretching program can reduce the chances for pathological GIRD, total arc range of motion deficit, time lost from sport, and poor performance (2,8). We note two stretching techniques in the pictures below.

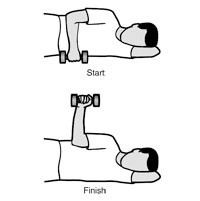
The Sleeper Stretch for the Post Capsule & IR
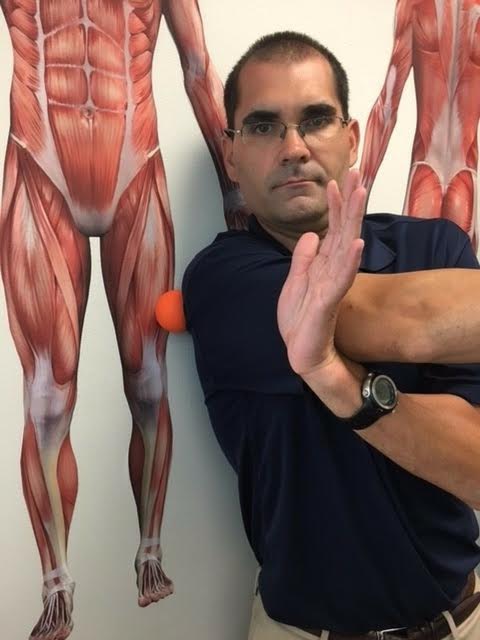
Self MFR/Self Mob for the Post Capsule
Manual therapy can be added to a daily stretching program to help further facilitate increased motion, reduce risk and improve performance. A small sample of some of the manual therapy options can be found in this linked video (https://www.youtube.com/watch?v=d55GsP_HjJs&t=18s).
The pictures below represent a case study. This is the internal rotation of my own R throwing shoulder. Years of playing baseball, throwing a football and other overhead activities created stiffness in my R throwing shoulder. The picture on the left is the initial amount of internal rotation of my R shoulder. The picture on the right side is the post-assessment. The clinician performed glenohumeral posterior and inferior mobilization for several minutes and an internal rotation post-isometric relaxation (PIR). You can see the drastic difference that treatment can make in a short amount of time.


Pathology vs. Morphology
We must truly differentiate pathological changes in the shoulder and elbow in overhead athletes from normal and expected wear and tear. Repetitive overhead mechanics create degenerative changes, which are very evident on routine and advanced diagnostic imaging like MRI, CT and diagnostic ultrasound.
The rate of degenerative changes is somewhat high. In the past, the presence and the rates of overhead athletes with degenerative changes significantly influenced our medical decision making, particularly, who was and wasn’t a candidate for more advanced options like injections and surgery. However, it should be noted the outcomes may not have been any better.
The abuse of imaging, coupled with subpar outcomes, led the medical world to develop the ironic radiological acronyms “BARF” and “VOMIT.” “BARF” is the acronym for “baseless application of radiological findings.” “VOMIT” is the acronym for “victim of modern imaging technology.” Essentially, health care providers were overemphasizing the diagnostic imaging findings without correlating the imaging findings to the patient’s actual clinical presentation. Decisions on medical interventions, namely the more aggressive options like medications, injections, and surgery, were erroneously made based on these deemed pathological rather than morphological entities. Effectively, this aberrant decision making sabotaged the chances for excellent outcomes.
Four studies highlight this point:
1. The first study looked at pre- and post-MRI of asymptomatic shoulders in overhead athletes with a 5 year follow up. The study found 40% had a rotator cuff tear, with 25% having a Bennett lesion (glenoid mineralization). None of the athletes 5 years later had subjective symptoms or required additional management. The conclusion of the study was, “MRI alone cannot be used for decision making on operative management.”
2. The second study looked at X-ray findings of the shoulder and elbow of major league players. The study found that no single radiographic finding predicted status on the disabled list. The number of shoulder and elbow degenerative findings correlated to the number of innings pitched. The conclusion of the study was, “Professional pitchers develop degenerative changes over time in both the shoulder and elbow of their dominant (pitching) arm due to chronic repetitive stress placed across the joints. These findings do not predict time spent on the Major League disabled list.”
3. The third study looked at elbow MRI findings and their relationship to the disabled list in asymptomatic professional baseball players. The study found that MRI findings in asymptomatic pitchers were not associated with placement on the disabled list within 1 year. Structural changes followed a predictable pattern on MRI. The main conclusion was, “Abnormal findings on MRI, even high-grade partial UCL tears, do not correlate with near term placement on the DL, mitigating their potential negative impact on signing decisions.”
4. The fourth study looked at glenohumeral findings on MRI and innings pitched in asymptomatic pitchers. The study found that 11 out of 21 and 13 out of21 pitchers had either a rotator cuff tear or a labral tear. A strong relationship existed between the presence of a rotator cuff tear or labral tear and number of innings pitched. The conclusions were, ‘MRI findings do not appear related to future time on the DL and that asymptomatic shoulder lesions in professional baseball pitchers appear to be more frequent than previously thought.”
The final word on pathology vs. morphology appears to be that degenerative changes should be considered the norm, and our interventions should be based on the clinical presentation, not solely on imaging findings.
The Scapula
The scapula serves as a key link between the lumbar spine, thoracic spine, cervical spine, pelvis, rib cage and humerus. The scapula can cause problems in other areas of the kinetic chain or compensate for problems elsewhere. Force couples are critical to the scapula.
Force couples have the following roles:
1. Maintain the instant center (“centration”) of rotation of the glenohumeral articulation;
2. Provides and controls motion of the scapula along the thoracic wall;
3. Elevates the acromion during glenohumeral elevation to:
a. Maintain the scapulohumeral rhythm;
b. Preserve the subacromial space;
c. Prevent subacromial Impingement; and
4. Transfer force and load to interdependent regions in a task-specific manner.
The ideal combination of scapular movements in the overhead athlete during arm elevation is upward rotation, posterior tilt, and external rotation. These motions clear the acromion from the humerus, preserving the subacromial space. Key muscles that assist with this combination of movements are the serratus anterior and inferior trapezius.
The role of the scapula in the overhead athlete was recently discussed in great detail at the 2013 Scapula Summit. The topic of scapular dyskinesis was of importance. Scapular dyskinesis is an alteration of the normal position or motion of the scapula.
Conclusions of the summit were (10):
1. Scapular dyskinesis is present in a high percentage of most shoulder injuries;
2. The exact role of the dyskinesis in creating or exacerbating shoulder dysfunction is not clearly defined;
3. Shoulder impingement symptoms are particularly affected by scapular dyskinesis;
4. Scapular dyskinesis is most aptly viewed as a potential impairment to shoulder function;
5. Treatment strategies for a shoulder injury can be more effectively implemented by evaluation of the dyskinesis;
6. A reliable observational clinical evaluation method for dyskinesis is available; and
7. Rehabilitation programs to restore scapular position and motion can be effective within a more comprehensive shoulder rehabilitation program.
The summit also discussed the concept of the SICK Scapula Syndrome (10). “SICK” stands for:
1. Scapular malposition
2. Inferior medial scapular winging
3. Coracoid process tenderness
4. Scapular Dyskinesis
Scapular malposition is noted in a general postural observation and by comparing side to side reference points, such as the acromions, coracoid processes, superior angles, inferior angles and medial borders of the scapulae. Inferior medial scapular winging is noted in static analysis on the medial border, as well as dynamic movement analysis looking at scapular motion during arm elevation. Coracoid process tenderness is based on palpation of the attachment of the pec minor onto the scapula. Scapular dyskinesis is noted with dynamic observation of the scapula during flexion and abduction, as well as the special tests of scapular assistance and scapular repositioning.
Dynamic Assessment of the Scapula: Scapular Assistance & Repositioning Test
The scapular assistance test assists the scapula into a posterior tilt, upward rotation or a combination of both. The test seeks to reduce symptoms such as shoulder pain, often linked with subacromial impingement. Theoretically, the examiner’s hands facilitate the scapular stabilizers of the inferior trapezius and serratus anterior assisting in a posterior tilt, upward rotation, or both movements combined, depending on the movement and pattern tested. In the pictures below, the examiner helps the subject into upward rotation during arm abduction, looking for a change in reported symptoms.


Examiner finds the inferior angle of the scapula Examiner assists the scapula during arm elevation
The scapular repositioning test places the scapula into external rotation and posterior tilt. The test compares baseline orthopedic test results, strength and pain-free motion findings to findings after the scapular repositioning occurs. Improved orthopedic test results, increased strength and increased pain-free motion during the repositioning maneuver indicate that scapular stability and improved neuromuscular control is warranted in the patient’s treatment plan. In the picture below, the empty can maneuver is tested in the scapular plane with and without the repositioning maneuver. A positive test would indicate increased strength to manual muscle testing, with less reported subjective pain.


The Overhead Athlete’s Elbow
Dr. Neil ElAttrache, M.D., of the Los Angeles Dodgers, said the following on the ulnar collateral ligament (UCL), “There is no ulnar collateral ligament that is strong enough to throw a ball over 90 miles per hour repeatedly. So the shielding of the ligament with perfect body mechanics and perfect muscle forces all have to be working perfectly. If they’re not, that sudden exposure to that kind of force will tear the ligament.” (11) Dr. ElAttrache is also quoted as, “If you ruptured the ligament God gave you, you can tear the one we’re going to give you.” This is a bit of harsh reality toward pitchers from a skilled expert.
UCL injury as described in the opening of this article is on the rise in youth overhead sports, particularly baseball. Some physicians have even reported a ten-fold increase since 2000. Youth athletes have less of a chance of recovering from this procedure than professional players. Estimates indicate that 25-30% of the young people under 18 years of age aren’t playing baseball after UCL reconstruction vs. professional baseball players that have a return to sport rate of > 80% (13, 14).
The throwing motion creates stress to the medial elbow, lateral elbow and posterior elbow as noted below (15). The medial elbow undergoes tremendous distraction forces, subjecting the UCL to potential stretch or tearing injury. The lateral elbow suffers compressive forces, increasing the chance for degenerative changes, such as reactive bone spurs. The posterior elbow receives tensile, compression and torsional forces leading to valgus extension overload. The valgus extension overload is implicated in osteophytes, stress fractures, and physical injuries. These mechanisms need to be understood and thoroughly evaluated in the overhead athlete.
Evaluation of the Overhead Athlete
Critically important is a simple yet thorough evaluation of the overhead athlete. The evaluation should consider both structure and function. It should consist of static assessment and dynamic assessment, including orthopedic testing and functional movement assessment. This short video covers the pertinent exam components https://www.youtube.com/watch?v=FG_g25HhYws&t=2s.
Rehab Considerations in The Overhead Athlete
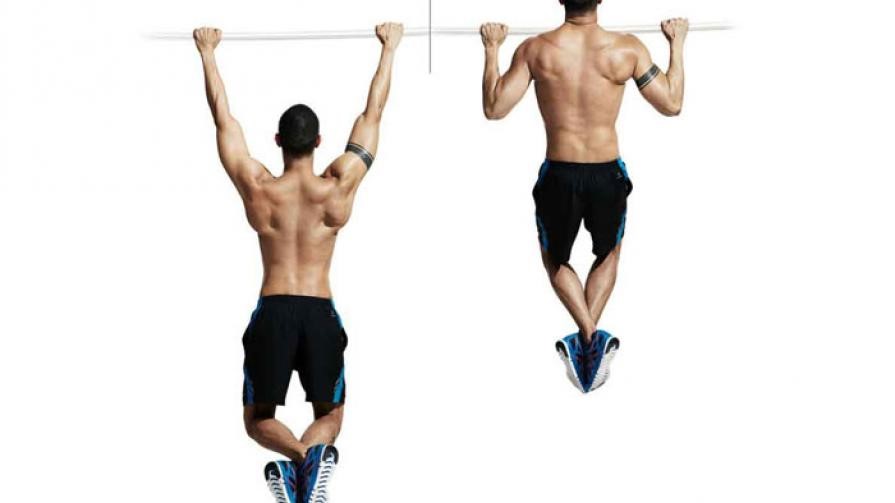
It is clinically important to train movements and patterns, rather than muscles in isolation, in the overhead athlete. Some muscle firing patterns may be “useful” for one movement and “aberrant” in others; therefore, exercise prescription to target a muscle with a template or protocol could undermine your long-term objectives. For years, the gold standard of upper extremity rehab was the “Thrower’s Ten” protocol (9). Some components were later replaced by the Blackburn protocol (9–Pgs 3 & 4).
The “Thrower’s Ten” protocol utilizes mostly open kinetic chain exercises thought to “activate” and “strengthen” the scapular and rotator cuff muscles. The Blackburn protocol focuses on open chain scapular exercises. Initially, it was believed that if the exercise produced high levels of activation on EMG, then the muscles were “working” to support and protect the shoulder and that high levels of activation indicated the exercise was doing what we thought it should do. It was believed that high levels of EMG activation meant better exercise. It was believed that the exercise would also have direct carryover into the athlete’s sport-specific overhead movement.
Humbly, I regret to say that I subscribed to the protocol mentality. I have a history of working with collegiate and professional overhead athletes. The “Thrower’s Ten” and Blackburn protocols are very entrenched in those settings. Those protocols guided my exercise prescription for years. Unfortunately, I had athletes and patients that did not respond as expected to the indicated protocols. Count me in as one of the formerly trusting subscribers to the protocol mentality.

In the above picture, I’m performing the Blackburn “T” Exercise. The cues here are to retract (“pinch”) the shoulder blades together while bringing the arms level with the torso, keeping the palms facing forward toward the ground. Notice how my R and L scapulae are overtly retracted and “winging.” There is significant increased tone in bilateral levator scapulae, bilateral upper trapezius and bilateral rhomboids (major & minor). This is occurring despite the goal of the exercise to target the inferior trapezius and serratus anterior. Remember, scapular stability is accomplished when the shoulder blade is flush with the rib cage and thoracic spine. The ability to go flush provides the rotator cuff with better leverage and a better base from which to work on top. This creates the “centration” and “reflexive stability” that we discussed earlier.
The exercise above is not accomplishing its intended goal. In the past, I would prescribe this exercise as part of a protocol, thinking it was an “evidence-based” approach. It was “evidence-based” at the time; however, our conceptual understanding of UE mechanics has changed. I’ve had to keep up with the times and update my exercise selection and prescription practices to best serve my patients. A sample of some of the rehab exercises that I currently prescribe can be found in this link (https://www.youtube.com/watch?v=Imqo8ZmCDCs&t=5s). The exercises trace the process of taking the athlete from pain to performance.
Prevention of Injury in the Overhead Athlete
Perhaps the most important and undervalued part of treating the overhead athlete lies in avoiding the need to treat the athlete in the first place. That means prevention. That means “prehab.” If you have the chance, get the word out in the youth sports community that prevention strategies can be effective in reducing injury and even enhancing performance.
Research outlines 4 major risk factors for UE injury in overhead athletes (3,7,):
1. Pathological GIRD & total arc ROM deficit greater than 5 degrees;
2. External rotation ROM dominant side not greater than 5 degrees vs. non-dominant side;
3. Rotator cuff strength (side by side comparison and versus preseason baselines);
4. Scapular dyskinesis (scapular position, strength and dynamic adaptability); and
5. Total use/abuse (total # throws).
The strongest risk factor of the above grouping is total use. Total use is the total number of throws, including warm-up throws, practice tosses, and in-game pitches. All throws add cumulative wear and tear to the shoulder and elbow.
Consider implementing the following measures in the overhead athlete:
1. Maintaining symmetric side to side total arc ROM with a focus on internal rotation;
2. Build symmetric side to side rotator cuff strength and endurance;
3. Reducing scapular dyskinesis with a targeted & comprehensive prehab/rehab program; and
4. Monitor closely the number of throws and pitches.
The Final Word
I hope this information on overhead athlete injury is useful to you and your patients. Many of these injuries and surgeries are preventable. “Each one teach one.” Please take some of this information and teach it to another. Teach a parent. Teach a youth baseball coach. Teach a youth athlete. Let’s keep our kids out of the operating room and on the field!
References
1. http://ftw.usatoday.com/2014/07/tommy-john-surgery-youth-sports
2. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3414068/
3. https://www.ncbi.nlm.nih.gov/pubmed/23775245
4. https://www.ncbi.nlm.nih.gov/pubmed/237752
5. https://www.ncbi.nlm.nih.gov/pubmed/22311291
6. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4458919/
7. https://www.ncbi.nlm.nih.gov/pubmed/26537804
8. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5366891/
9. http://athleticmed.com/wp-content/uploads/sites/2/2013/10/Throwers_Ten_Exercise_Program.pdf
10. http://bjsm.bmj.com/content/47/14/877.long
12. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3435939/










{kind=link}