




Radiology of Hemophilia

Hemophilia is a congenital disorder in which there is an absence of a specific blood clotting factor. In a patient who suffers from this disease, even relatively minor trauma may induce bleeding, which, because of the absence of a clotting factor, may continue. This may occur in many tissues of the body; however, radiographically this is manifested in the skeleton and joints.
The gene for hemophilia is carried by the female but does not manifest symptoms in the female. It can, however, be transmitted to a male offspring in which symptoms do develop. There are two main types of the disease that result in skeletal abnormalities. Classic hemophilia is a lack of clotting factor VIII and is termed “hemophilia A.” Lack of clotting factor IX is termed “hemophilia B,” or “Christmas disease.”
Advertisement

As an interesting side note, perhaps one of the most famous transmissions of this disease is in the royal line of Queen Victoria of Great Britain in the late 19th and early 20th centuries. The queen was a carrier for hemophilia B. One of her granddaughters, Alexandra, was also a carrier of the disease. Alexandra married Tsar Nicholas the Second of Russia, and their son, Alexei, was stricken with the disease. Desperate attempts to heal the boy precipitated an association with a monk named Grigori Rasputin, a charlatan faith healer. Rasputin was able to quell some of the attacks of hemophilia and thus gain the trust of the royal family, particularly Alexandra. Rasputin proved to be an unsavory character, and the general Russian populace was not impressed with the close association of the family with the monk. This association may have been a factor in the fall of the Romanov dynasty and the subsequent rise of Bolshevism in Russia.
Clinically, in hemophilia, there is a broad range of symptom expressions. In some individuals, the episodes of hemorrhage are minor and infrequent, while in others, quite the opposite is true, and there may be bleeding in a number of different tissues. Sites of hemorrhage may include body cavities, bones, and joints. 80% of bleeding occurs in joints (1). This may be within the joint cavity, but also intraosseously as well.
Bleeding into the joint may initially result in no abnormality; however, with recurrent bleeding, there will be the initiation of pannus formation. There will follow articular adhesions and fibrosis of the joint capsule, with the deposition of hemosiderin in the synovium. With time there will be the destruction of the articular cartilage. Hemorrhage within the bone will result in cyst formation, localized bone resorption, and periosteal new bone. Epiphyseal overgrowth may result, as well.
A physical manifestation of this condition is soft tissue swelling. On x-ray there is epiphyseal osteoporosis as a result of the local hyperemia. Subarticular fluid deposits result in intraosseous cysts. This occurs most frequently in the lower extremities and hands, with the knee being the most frequent joint involved. When there is extensive hemorrhage in the bone, it may result in large expansile lucencies that are termed “pseudo-tumors.” This is seen most frequently in the ilium. The end result of a hemophilic joint may be severe degenerative change and intraosseous fusion.
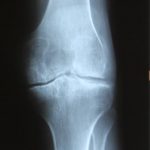
Images 1 and 2 demonstrate sequelae of repeated hemorrhages in the knee, with overgrowth of the medial femoral condyle and mild subchondral osseous destruction. The lateral view illustrates the distention of the joint with deposition of hemosiderin in the capsule and the dense appearance of the soft tissues. The patient represented in figure 3 demonstrates gross loss of joint spacing with sclerosis of the subchondral bone in the lateral compartment. Late-stage sequelae in the wrist are evident in figure 4, with a regional osteopenia and near-complete loss of intercarpal articular cartilage and degenerative fusion. Figure 5 exemplifies the pseudo-tumors that may occur with a large expansile, lucent lesion in the supra-acetabular region of the ilium.




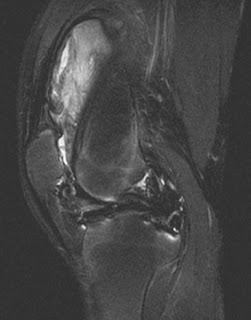
MRI images of the knee demonstrate gross loss of the hyaline articular cartilage, with cortical irregularity at the articular surface of the lateral epicondyle in figure 6, a T-2 weighted coronal image. Figure 7 demonstrates a large synovial mass in the suprapatellar pouch on this fat-suppressed sagittal image.

The appearance of hemophilia on plain film may resemble juvenile rheumatoid arthritis in young patients, and this distinction needs to be made in order to provide the appropriate treatment.
References
- Yochum T.R.,Rowe L.J.: Essentials of Skeletal Radiology, ed 3. Philadelphia, Lippincott Williams & Wilkins, 2005











{kind=link}