




MRI of the Knee Normal Meniscal and Cartilage Anatomy

The knee is a body part that is frequently studied with MRI. Meniscal tears are a fairly frequent occurrence in the knee. It is essential to have a good knowledge of the normal appearance of the cartilage and menisci with MRI before beginning to assess possible pathology.
MRI Signal Intensity
The basics of MRI signal intensity apply similarly to all MRI studies. Cortical bone is hypointense (dark) on all imaging sequences. Normal healthy menisci and ligaments are hypointense as well. Medullary bone is intermediate to slightly hyperintense in signal intensity on most sequences. Fluid, such as that seen in a knee joint effusion, will be hypointense on the T-1 weighted images and hyperintense (bright) on the T-2 and fat-suppressed images.
Advertisement

Typical imaging sequences used for the knee may include T-1 and T-2 sagittal and coronal images with T-2 axial images. A fat suppressed sequence is generally included and is most often used in the coronal plane.
Brief Review of Fat-Suppressed Images
I always like to begin my search pattern with a brief overview of the fat-suppressed images, since pathology is generally more apparent in that sequence. Neoplasms and bone marrow edema are generally well seen on these images, and, in fact, are sometimes difficult to visualize on the spin echo sequences alone. Even subtle bone marrow edema is usually detectable as increased signal intensity on fat suppression. Soft tissue swelling associated with ligamentous disruption is well seen on these images as well.
The menisci require the utilization of two planes for complete imaging. The coronal and sagittal planes used together will provide comprehensive imaging of the anterior and posterior horns of the menisci, as well as the meniscal bodies. Normal menisci are uniformly dark on all imaging sequences, with the possible exception of minor increased intrameniscal signal intensity in children and adolescents (1). This is the result of a blood supply to the meniscus that gradually recedes with aging. When mature, the meniscus will appear hypointense on all sequences. The anterior and posterior horns are well visualized in the sagittal plane, while the meniscal bodies are best seen on the coronal images. Figure 1 is a representative sagittal image, which allows visualization of the horns. To view the transition between the body and horns of the meniscus requires correlation between the sagittal and coronal images. Figure 2 is a coronal image and demonstrates the bodies of the medial and the relatively smaller lateral meniscus.

Figure 1 
Figure 2
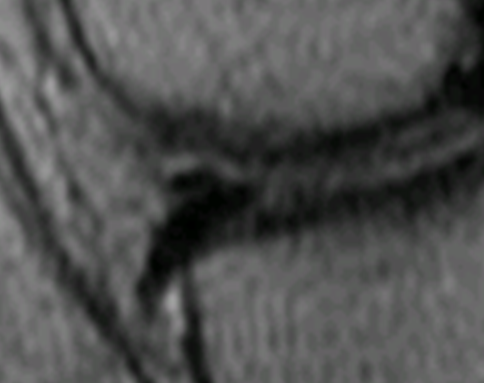
The meniscus is wedge-shaped in cross-section, with the apex directed into the center of the knee joint. The medial meniscus is generally larger than the lateral meniscus and is C shaped in configuration, while the lateral meniscus is more oval-shaped. The relatively larger medial meniscus is demonstrated in figure 2. Anteriorly, the horns of the menisci are connected by the transverse ligament. This ligament stretches across the intervening intercondylar region. When seen on the sagittal images, this ligament separates from the meniscus and should not be mistaken for a torn meniscal fragment (2). Figure 3 demonstrates the transverse ligament as an oval-shaped hypointense focus adjacent to the superior surface of the anterior horn of the meniscus in this magnified sagittal image. The posterior horn of the meniscus tapers to the meniscal root, which inserts on the tibia. This area is often overlooked and should be closely examined for tear.
The menisci are anchored to the joint capsule via the coronary ligaments. These stretch from the superior and inferior corners of the periphery of the meniscus to the lining of the joint capsule, and, in the case of the medial meniscus, the medial collateral ligament. The apex of the meniscus lies as a free edge within the joint.
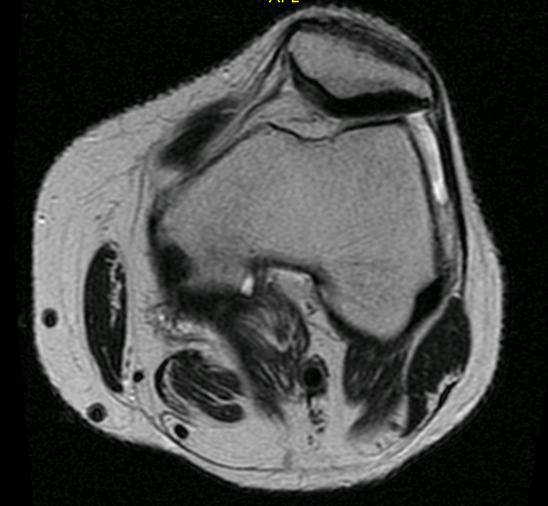
The joint spacing in the medial and lateral compartments of the knee is well seen on the coronal images. In figure 2 the cartilage is intermediate in signal intensity, with a thin line of hypointense joint fluid separating the femoral from the tibial hyaline cartilage on this T-1 weighted image. Cartilage should be of fairly uniform thickness and display somewhat intermediate signal on the T-1 images and is somewhat hypointense on the T-2 images. Areas of hyaline cartilage thinning (attenuation), as well as any overt chondral or osteochondral defect, can readily be seen. Patellar cartilage on the dorsal surface is of particular interest as it relates to chondromalacia patella. The axial images provide good visualization of this cartilage. Figure 4 demonstrates normal cartilage thickness at the dorsal surface of the patella on this T-2 weighted axial image. Uniform thickness and signal intensity in this area, with a lack of any underlying subchondral bone signal alteration, should be seen.
The menisci account for a large percentage of the abnormalities noted in the knee. The concept of meniscal tear will be explored in a subsequent article.
References:
1. Kaplan P. A. et al. : Musculoskeletal MRI, ed 1. Philadelphia, W. B. Saunders, 2001.
2. Stoller D. W.: Magnetic Resonance Imaging in Orthopaedics and Sports Medicine, ed 2. Philadelphia, J. B. Lippincott Company 1993.










{kind=link}