




MRI Appearance of Adhesive Capsulitis
Adhesive capsulitis (AC), or “frozen shoulder syndrome,” represents a fairly common cause of shoulder pain and restricted shoulder movement. Estimates place the frequency of AC in the general population at 3% (1). A higher percentage is seen in diabetic patients, ranging from 10% to 20%. Indeed, anecdotally the frequency of occurrence of this disorder seems to be increasing in the present day. The condition is more common in females, most often in the 40-70-year age group. Although usually self-limiting, it can result in a persistent debilitating disorder that greatly limits the activities of daily living. While plain film x-ray examination is found to be unremarkable, other modalities, such as arthrography and MRI, do provide findings that are diagnostic of this ailment. In this article, we will focus on the findings of non-arthrographic MRI.
To begin, let us briefly review a few salient points about adhesive capsulitis. The physical findings consistent with the condition are a painful restriction of both active and passive shoulder range of motion. A list of differential diagnoses would include impingement syndrome, rotator cuff pathology, and osteoarthritis. Less likely differentials might include nerve injury with neuromuscular dysfunction and cervical spine discopathy with radiculopathy. Indeed, rotator cuff pathology is frequently seen in conjunction with AC.
Advertisement
Primary or idiopathic AC has no history of predisposing factors. Secondary adhesive capsulitis may be associated with a previous injury or surgery. Imaging findings for both types are identical. The underlying pathology is chronic inflammation of the inferior aspect of the joint capsule. There is thickening of the axillary pouch of the inferior glenohumeral joint capsule. The inferior aspect of the capsule is formed by the inferior glenohumeral ligament. Synovitis of the capsule develops and may be accompanied by joint effusion.
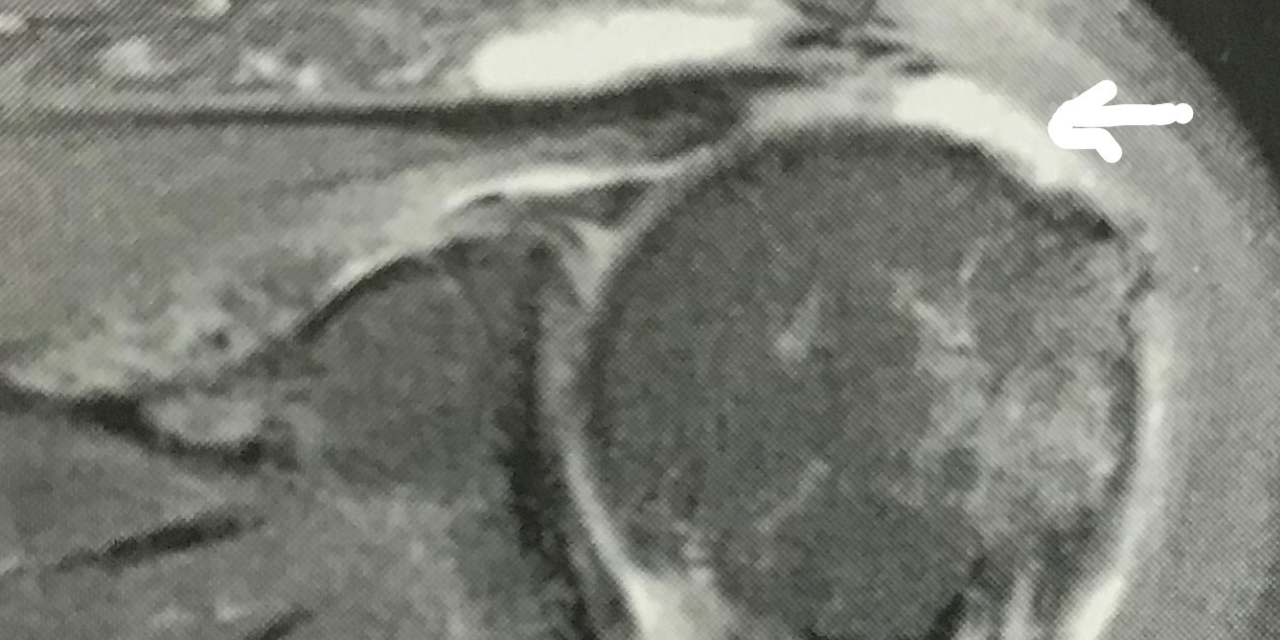
On MRI the appearance of the inferior joint capsule is one of thickening and a generally indistinct appearance. The margins of the capsule may appear fuzzy. Figure 1, a sagittal T-2 weighted image, demonstrates the normally well-defined non-thickened inferior joint capsule (joint fluid appears as hyperintense white signal extending down along the joint to the capsule). Note the well-defined inferior border (arrow). Contrast that image with figure 2, which shows the inferior capsule as thickened, with an increase in signal intensity on this STIR weighted sagittal image. Figure 3 demonstrates adhesive capsulitis that is concurrent with a torn rotator cuff tendon. The arrow indicates the gap left in the tendon that is now filled in with high signal intensity fluid on this STIR sagittal image. There has been retraction of the musculotendinous junction. The inferior joint capsule is poorly defined, intermediate in signal intensity, and grossly thickened.



MRI is an excellent tool for the confirmation of this condition and has the added advantage of demonstrating concurrent shoulder conditions, such as rotator cuff pathology. Plain film x-ray is of limited use in diagnosing AC, other than to rule out conditions such as degenerative osteoarthritis. Unfortunately, adhesive capsulitis may accompany osteoarthritis which, may muddy the picture.
Fortunately, this condition often responds well to conservative chiropractic care consisting of passive stretching, joint manipulation, and soft tissue manipulation. Patients recalcitrant to conservative measures may benefit from manipulation under anesthesia or arthroscopic capsular release.
References
- Stoller D. W.: Magnetic Resonance Imaging in Orthopaedics and Sports Medicine, ed
- Philadelphia, J. B. Lippincott Company 1993.











{kind=link}