




Top 5 Masqueraders of Osseous Disease on Radiographs
There are several non-pathologic findings on radiographs that may cause concern for clinicians who are not familiar with them. Based on my experience as a chiropractic radiologist, these are the five most common osseous findings that often raise questions from clinicians. It is my goal to familiarize the clinician with the appearance of these findings to avoid any unnecessary further imaging ortesting, ensuring the best experience and care for the patient.
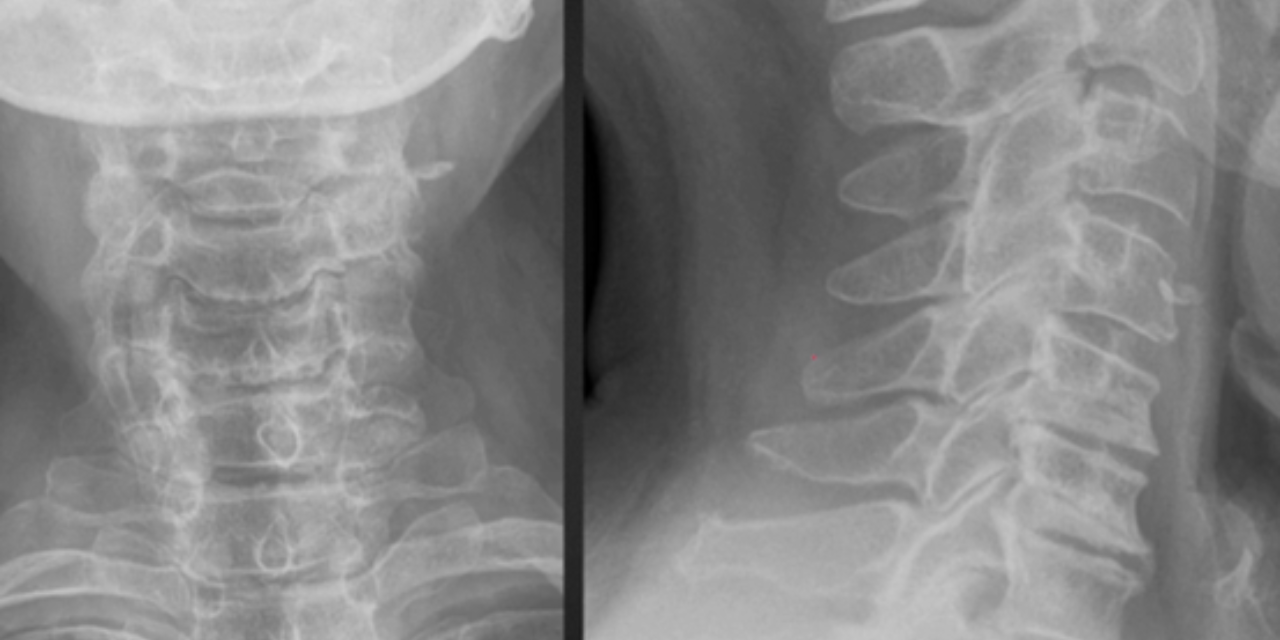
1. The Pseudofracture Appearance of Uncovertebral Arthrosis
In the lateral view of figure 1, note the horizontal radiolucent line through C5 and C6. This finding is often mistaken for a fracture on radiographs. The AP radiograph nicely demonstrates uncinate process hypertrophy at C6 and C7. The degenerative hypertrophy of the uncinate processes causes an abnormal pseudoarthrosis to form between the uncinate process below and the inferior vertebral body above. This pseudoarthrosis results in the horizontal radiolucency seen traversing the vertebral body.
Advertisement

2. Limbus Bone
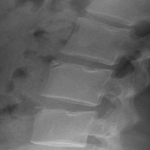
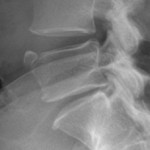
A limbus bone is an unfused secondary ossification center of the vertebral body (typically the anterosuperior corner), due to herniation of the nucleus pulposus through the ring apophysis prior to skeletal development. This fragment remains ununited to the vertebral body throughout the patient’s life. This can be differentiated from a fracture in that it is well-corticated, triangular, and the fragment of bone will not exactly “fit” into the defect. These fragments may be smaller than the defect of the bone (figure 2) or they may hypertrophy over time and become larger (figure 3). A limbus bone is most often asymptomatic.
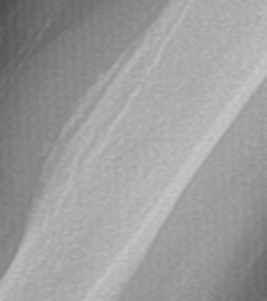
3. Prominent Soleal Line


Figure 4 demonstrates prominent ossification that obliquely traverses the proximal tibia at the origin of the soleus muscle. Figure 5 demonstrates a thick osseous protrusion along the posterior tibia. This normal variant can be mistaken for an aggressive periosteal reaction or pathologic heterotopic ossification. But the anatomic orientation of the ossification along the soleal insertion and no involvment of the underlying bone should allow the clinician to easily identify this variant. This normal viariant has also been termed tibial pseudoperiostitis or tibial tug lesion.
4. Pseudotumor Deltoideus

This normal variant appears as a prominent deltoid tuberosity with cortical radiolucency and irregularity. This finding occurs due to the insertion of the deltoid tendon at the deltoid tuberosity. This non-pathologic anatomic variant can be confused with malignancy, due to the irregular lucent appearance and the simulation of an aggressive periosteal reaction. A knowledge of the classic location and appearance should allow for proper diagnosis and avoidance of unnecessary imaging or biopsy.
5. Synovial Herniation Pit


This non-pathologic radiolucency is seen in up to 5% of the adult population and is most often asymptomatic, though symptomatic cases have been described. The classic appearance is a round, ovoid, or “8-shaped” radiolucency with a thin sclerotic border most often found at the anterior superior femoral neck, though it can be found in the anterior inferior femoral neck as well. It is formed by a herniation of synovium through a cortical defect of the femoral neck. They are usually 5-mm or less in diameter and are more often found unilaterally than bilaterally.











{kind=link}