




The Imaging Appearance and Possible Clinical Consequences of the Os Odontoideum

The os odontoideum is one of many developmental abnormalities that can occur and yet be completely occult to the examining physician. Imaging is the only way to reliably diagnose this condition. If this condition goes undiagnosed and chiropractic manipulation to the cervical spine is performed, there is the possibility of severe consequences.
The os odontoideum, as mentioned previously, is a developmental abnormality. This differs from a congenital anomaly in that a developmental condition is acquired and not present from birth. During development the dens ossifies separately and fuses to the body of C2 between the ages of 5 and 7 years. Os odontoideum represents non-union of the dens from the body of C2. Current theory supports trauma during early childhood as the inciting factor responsible for the separation of this ossicle. The transverse ligament usually remains intact. There may be an underlying predisposition in some cases for the formation of this condition, however, as there has been reported increased incidence with Downs syndrome, occipitalization, atlas hypoplasia, block vertebra, Klippel-Feil syndrome and skeletal dysplasias (1).
Advertisement
The majority of patients with this condition are asymptomatic and in these cases, there is generally no physical finding. The condition is usually diagnosed incidentally in these patients when a cervical spine study is obtained for other reasons. In some patients, torticollis may be present clinically when there is atlantoaxial subluxation. Suboccipital pain and neuralgia, audible crepitus and a jerky movement on flexion/extension may be present as well.
Atlantoaxial instability is a contraindication to high-velocity manipulation at the C1-C2 level. The danger of adjusting this area is the possibility of precipitating a compression syndrome of the cervical cord or brainstem. There also exists the possibility of vascular injury. The spinal arteries or vertebral arteries may be involved and result in vertebrobasilar artery, cerebellar artery or ventral cord syndromes. Even in presumably asymptomatic cases, there remains the possibility of vascular, cervical cord or brainstem damage as a result of manipulative therapy.

This condition may be identified on the AP open mouth view or less commonly on the lateral view. The ossicle is round or ovoid in shape and there may be significant separation between the ossicle and the subjacent body of C2 (figure 1). The ossicle is typically well corticated. Since the transverse ligament typically remains intact, the anterior arch of C1 moves in unison with the ossicle. Hypertrophy of the anterior arch of C1 with a sclerotic appearance may be present in the adult. The observation of this appearance will help to exclude an acute dens fracture. In some cases the os is difficult to identify on any of the cervical spine projections and a diagnosis of odontoid agenesis may be misdiagnosed. Sectional imaging (CT or MRI) will identify the os if there is any question on the plain films.
When an os odontoideum is identified, flexion and extension lateral cervical projections must be obtained to assess for instability at C1-C2. Instability in the cervical spine is defined as greater than 3.0 mm of AP translation on the stress projections. This may be measured using the spinolaminar lines of the C1 and C2 posterior arches and noting the amount of combined translation from flexion to extension (Figures 2 and 3).

Figure 2 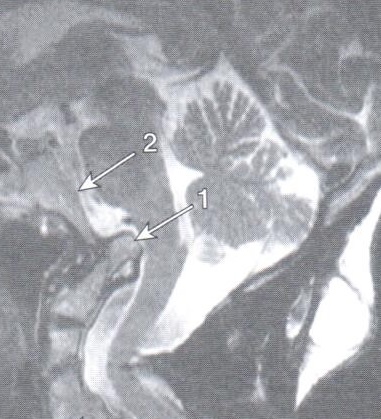
Figure 3
MRI examination is helpful in assessing the condition of the spinal cord. Cord contusion or myelomalacia may be detected (figure 4). In this example, there is an area of cord myelomalacia at the level of the dens defect. MRI can also be used to estimate the possibility of instability based upon the appearance of the tissue between the ossicle and the underlying body of C2. The hyperintense signal on the T-2 weighted image in the defect of figure 4 is indicative of instability. Fibrous tissue will manifest hypointense signal within the defect, which suggests that the anomaly is stable. Figure 4 also reveals the hypertrophy of the anterior arch of C1 that may occur with os odontoideum.

In conclusion, os odontoideum is a condition that may be a contraindication to high-velocity manipulation of the upper cervical spine. If you are looking for a good reason to x-ray patients in which you will be adjusting the upper cervical spine, you just found one.
References
- Yochum T.R., Rowe L.J.: Essentials of Skeletal Radiology, ed 3. Philadelphia, Lippincott Williams & Wilkins, 2005











{kind=link}