




Achilles Tendon and Calf Injuries: One and the Same

By Dr. Adam Rodnick, DC
One of the biggest recent sports stories involved Kevin Durant of the Golden State Warriors. In game 5 of the NBA Championships in Toronto, Canada, Kevin went down with an Achilles tendon injury.1 The interesting situation here is that Durant had also been nursing a calf injury for the previous few weeks that actually kept him out of the first 4 games of the NBA Championship. It was hard watching him fall to the ground, clutching his right Achilles and calf area with his hands. He limped off the court assisted.
Advertisement

As people looked for answers to what had happened, Bob Meyers, the President of the Warriors, spoke at a press conference after the game. He stated, “The initial injury was a calf injury. This is not a calf injury.” Myers said, “I’m not a doctor, I don’t know how those are related or not, but it’s a different injury.”2
This is an opportunity to discuss the general public’s lack of knowledge of the lower extremity anatomy, biomechanics, movement patterns, and how they are all related. One of the most frustrating things for me in active practice is how little education our patients are given about their own bodies, including the feet, ankles, legs, and knees. It’s time to break down the Achilles tendon and calf relationship, as almost all health care providers deal with this area frequently in clinical practice.
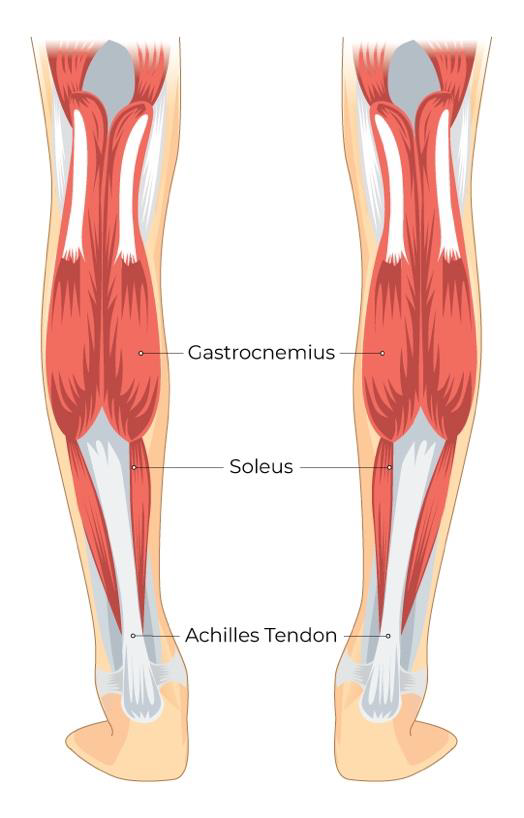
The Calf
The calf is often referred to as “Sura,” which is the Latin word. It is the back portion or posterior compartment of the leg. The two largest muscles (the gastrocnemius and soleus) are known together as the calf muscles, and they both attach to the calcaneus bone via the Achilles tendon.3
Understanding the anatomy of the calf is pretty simple, so let’s complicate things a bit. If you recall, we all have 3 functional arches on the bottom of each foot; The medial longitudinal arch, the lateral longitudinal arch, and the transverse (metatarsal) arch. These three arches form the plantar vault, and it is the basis for stability for the human foot. The arches are formed by the plantar fascia and the bone to bone ligaments (like the spring ligament). When the arches are working well, the foot is allowed to move fluidly into regular pronation, regular supination, and proper weight-bearing during standing and the gait cycle.
Up to 99% of the population display excessive pronation, where their arches flatten out too much and fall towards the ground.4 Because this phenomenon happens so frequently in the patients who come to us for care, it is easy to see daily. When the feet are over-pronating, the three arches drop more than they should. As the foot falls to the ground, the tibia bone must inwardly rotate as a compensatory mechanism. The inward rotation of the tibia then causes the femur to rotate inward (medially) as well.
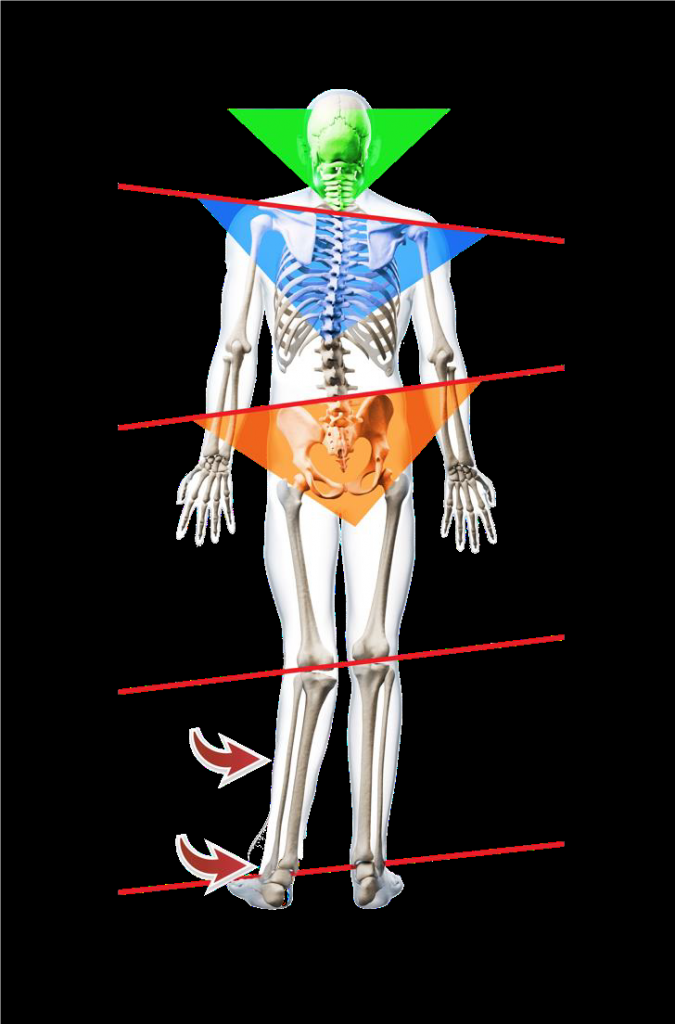
The excessive pronation has now set up a biomechanical situation where the dropping of the arches and inward rotation of both the tibia and femur bones stress the inner ankles and knees. As one of the consequences of this, the gastrocnemius and soleus muscles are over-contracting, even at rest. Muscles that are essentially getting overworked are very susceptible to injury and damage. We can see this damage range from a “calf strain” or “pulled leg muscle” all the way through to “Achilles tendonitis, “Achilles tendon tears” or “complete ruptures.”
It’s not just that the gastrocnemius, soleus, and Achilles tendons are located to close to one another. The physical relationship is compromised by the biomechanical fact that excessive foot pronation can and will negatively affect the forces coming up from the heel and ankle into the Achilles tendon and calf. This relationship is what most people don’t understand.
So the question arises: What can I do in my clinic when an Achilles tendon/Calf injury patient presents?
- Evaluate the lower extremity properly! Have the patient take off their shoes and socks and stand in front of you in anatomical position. You will clearly see how flat their feet are (Look for the 5 signs of foot pronation). Often, you will see the tibia and femur bones internally rotating and how tight and hypertonic the calf muscles and Achilles are on one or both sides.
- Utilize appropriate physiotherapy modalities like cold laser, ultrasound, EMS, and/or a host of other modalities that will help the patient whether they are acute or chronic. Soft tissue techniques (ART, Graston, etc.) are also very useful in helping those muscles and soft tissues improve.
- Administer chiropractic adjustments to all 26-foot bones, the tibia, femur, and fibula. Since most patients presenting to our clinics are excessive foot pronators, the listings of all these bones are in quite a predictable pattern. It is easy to know what to look for and how to adjust it.
- Utilize custom, three-arch, flexible foot orthotics. Once the plantar fascia stretches past a certain point, the arches fall and the foot will continue to flatten out. Having the right type of orthotics support all 3 arches giving the foot, and therefore the body, a stable base of support. If one does not support the arches, the over-pronation will continue to stress the calf muscles and the Achilles.
- Ensure the proper footwear. Athletic, dress, and casual shoes must be inspected by you, the doctor, so you can assess if they work well with the custom orthotics and provide solid support for the patient. Many patients wear shoes that are so bad, they help create the stress to the ankle and knees. Some shoes are so unsupportive they won’t even work with any orthotics.
- Give home care instructions that can include stretching and strengthening exercises of the calf and foot. Discuss appropriate activities to keep them active but do not aggravate their condition. You may have to take a patient off their sport short term while you get them stabilized and make sure their feet are supported well.
You may never see a patient of the caliber of athlete that Kevin Durant is. But your patients deserve you treating them like they are a superstar. Please take the time to look at their feet, ascertain their pronation degree and treat them properly. Foot support is key or else the over-pronation pattern will continue having a field day with stressing out your ankle, knee and the muscles located in that area. Plus, your adjustments of the ankle and knee will never truly hold unless the three arches are supported properly.
References:
1. Kevin Durant injury update: Warriors star undergoes surgery for ruptured Achilles tendon. https://www.cbssports.com/nba/news/kevin-durant-injury-update-warriors-star-undergoes-surgery-for-ruptured-achilles-tendon/
2. Kevin Durant suffered Achilles injury, Warriors GM Bob Myers announces https://news.yahoo.com/kevin-durant-suffered-achilles-injury- 041444288.html
3. https://www.webmd.com/fitness-exercise/picture-of-the-calf-muscle#1
4. 99% of the population overpronates. https://www.footlevelers.com/overpronation











{kind=link}