

Fall and winter collision sports like football, hockey, and even soccer, pose unique threats to the bodies of its participants. The foot and ankle are common sites of injury. This article will focus on the current evidence-based assessment and management of one of the more troublesome ankle injuries.
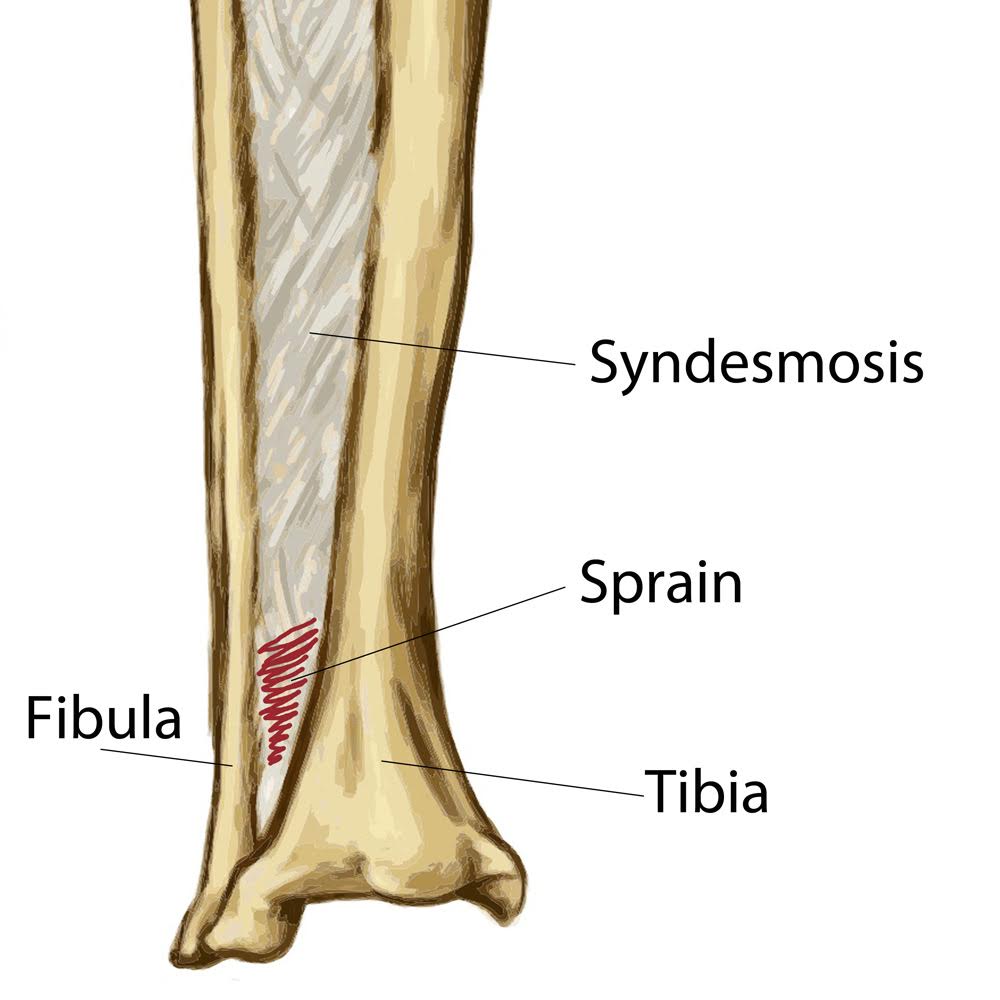
“Syndesmotic ankle sprain” or “high ankle sprain” follows damage to the ligaments and tissues that hold the tibia and fibula together at the ankle mortise joint. Syndesmotic sprains are much less common than their lateral counterparts (representing less than 10% of all ankle sprains) but are more difficult to assess and manage with significantly longer recovery times. (1-3)
Advertisement

Joint Anatomy
The ankle mortise joint is comprised of the (slightly concave) tibia and the (slightly convex) fibula, which rest on the talus. (4,5) These three bones are held together by three ligaments: the anterior tibiofibular ligament (AITFL), the posterior tibiofibular ligament (PITFL), and the interosseous membrane. The triangular-shaped AITFL begins with a broad origin on the anterolateral tibia and runs obliquely to a point on the anterior aspect of the lateral malleolus. (5-7) The more horizontally oriented PITFL is comprised of a superficial band and a deeper component (inferior transverse ligament) that together connect the posterior aspects of the tibia and fibula. (5,7) Finally, the interosseous membrane connects the medial aspects of the tibia and fibula along their entire length. (4) The distal termination of the interosseous membrane consists of a fibrotic thickening, called the interosseous ligament, which further stabilizes the joint. (6,9)
The primary function of the syndesmotic ligaments is to prevent excessive widening of the ankle mortise by holding the fibula tight to the tibia. (10) During normal ankle dorsiflexion, the wider anterior aspect of the talus wedges and spreads the tibia and fibula by 1-2 millimeters. (10,11) Additionally, ground reactive forces cause approximately 5 degrees of external rotation of the talus, which forces the fibula laterally. (10) The distal fibers of the interosseous membrane act in a spring-like fashion to accommodate this separation during dynamic loading.
The Injury
Disruption of the syndesmosis occurs from forces that cause excessive mortise widening, particularly external rotation (pushes the fibula laterally) and hyperdorsiflexion (wedge effect). (11,13-17) Isolated external rotation injuries produce a predictable pattern of damage, commensurate to the force involved. First, the deltoid ligament is ruptured (or the medial malleolus is avulsed), followed by progressive tearing of the AITFL, the PITFL, and finally, the interosseous membrane. (18) Particularly forceful injuries may terminate in a spiral fracture to the proximal fibula (Maisonneuve fracture). (18)
Symptoms
Patients typically present following an athletic injury that involves external rotation of the tibia on a planted dorsiflexed foot. (13) Syndesmotic sprains are common in collision sports, like football, hockey, and soccer. (12,14,19,20) Snow skiers may be predisposed from excessive rotational stress. (15) Symptoms may mimic those of other types of ankle sprain, but the pain of a syndesmotic injury is typically located slightly higher, just above the ankle. (21,22) Patients with severe injuries will not be ambulatory, and those able to bear weight will usually report pain when standing or walking. Dorsiflexion or outward rotation of the foot will likely intensify symptoms. Significant bruising or swelling is possible. Clinicians should suspect neurovascular compromise in patients complaining of numbness, paresthesias, or a cold foot. (23)
Palpation will likely demonstrate tenderness and swelling over the AITFL, but focal tenderness does not necessarily indicate injury to that ligament since AITFL tenderness is a common finding in any ankle sprain. (24) Tenderness that begins over the AITFL and extends proximally is a more noteworthy finding. The length of tenderness as measured from the distal tip of the lateral malleolus (Syndesmotic Tenderness Length) directly correlates with injury severity and disability for syndesmotic sprains. (25) Range of motion testing will demonstrate pain on dorsiflexion or external rotation. Passive external rotation with the ankle neutral or slightly dorsiflexed (External Rotation Test) widens the ankle mortise joint and will likely reproduce symptoms of syndesmotic injury. (14,25) A positive Eversion Stress Test may suggest Deltoid ligament involvement. Anterior and Posterior Drawer Tests may help assess for instability.
Tests
The Fibular Squeeze Test is a classic (but non-specific) assessment for syndesmotic injury that consists of compressing the mid-portions of the tibia and fibula to create sheer strain on the distal syndesmosis. (21,25,26) The test is considered positive when compression causes pain over the distal syndesmosis. A self-service version of the Fibular Squeeze Test called the Crossed Leg Test, is performed by having the patient cross the mid portion of the affected leg over the opposite knee while applying a compressive downward force over the proximal tibia. (27) The Syndesmotic Stabilization Test consists of applying athletic tape around the distal syndesmosis and having the patient perform the provocative activity, including standing, toe raising, heel raising, squatting, and jumping. Diminished pain with the ankle stabilized suggests syndesmotic injury. (25,28) Additional orthopedic assessments include translating the talus medially and laterally (Cotton Test) or sheering the fibula in an anterior to posterior fashion (Fibular Translation Test). (13,29-31)
Clinicians should assess for the possibility of neurovascular compromise by palpating the dorsalis pedis and posterior tibial pulses and testing sensation, particularly over the distribution of the sural and peroneal nerves.
Radiology
The Ottowa ankle rules are a well-established standard for determining the need for radiographs following trauma. (32-34) The Ottowa rules suggest that radiographs are appropriate following injury when there is point tenderness over the medial or lateral malleolus, navicular, and/or base of the fifth metatarsal or the instability to bear weight for at least four steps. Employing the Ottowa rules allows clinicians to exclude fractures with nearly 99% accuracy. (32-34) These rules were intended for adults, but have since been shown to be accurate for children as young as two years. (33,34)
Radiographic views would include AP, lateral, and ankle mortise views. Clinicians should observe for osseous avulsions on the anterior or posterior aspects of the tibia, which are present in up to half of all true syndesmotic injuries. (35) Stress radiographs, performed in a single-leg, weight-bearing position, may demonstrate widening of the ankle mortise joint. (25) Gapping of greater than 5 mm as measured on an AP or mortise view is considered “diastasis,” i.e., a pathologic separation of the ankle mortise joint. (7) This space is termed the “talofibular clear space.” Syndesmotic injuries may occur without diastasis, with diastatis that occurs under stress (i.e. weight-bearing radiographs), or frank diastasis. (36,37) A study on NHL hockey players demonstrated that only one out of 14 syndesmotic injuries demonstrated diastasis on stress radiographs. (38) MRI will definitively demonstrate ligamentous injury. Diagnostic ultrasonography can demonstrate ligamentous damage as well.
Highly suspicious cases, or those that do not respond to a short trial of conservative therapy, may require advanced imaging. (35,40) Advanced imaging is helpful to determine the grade of injury and to rule out alternate diagnoses, including osteochondral lesion or tumors. (10) A CT or bone scan may help detect subtler bony abnormalities (stress fracture, osteochrondral defect, etc.) (41) Dynamic ultrasound has been shown to reliably visualize AITFL tears or abnormal mortise widening. (10)
The differential diagnosis for syndesmotic sprain includes fracture (talar dome, calcaneous, malleolus, osteochondral, avulsion, etc.), intraarticular meniscoid (impingement syndrome), complex regional pain syndrome (RSD), tendinopathy (tibialis posterior, flexor hallucis longus, Achilles, peroneal, etc.), medial or lateral sprain, inflammatory arthoropathy, peripheral neuropathy, or osteochondritis dissecans.
Treatment
While ankles demonstrating diastasis or instability will likely require surgical intervention, most uncomplicated Grade I syndesmotic sprains will respond to conservative care. (42-48) However, syndesmotic ankle sprains heal more slowly than their medial and lateral counterparts. (49) In fact, recovery of a syndesmotic sprain may require a treatment period twice as long as a Grade III lateral ankle sprain. (10,38) Sports-specific disability can last up to four months with an average recovery time lasting between 2-7 weeks. (50)
Early Rehab
Early progressive rehab may help improve lymphatic drainage, enhance proprioception, restore ligament strength, and minimize fibrosis and atrophy. (25) The initial goals of treatment include suppressing pain, inflammation, and swelling while preserving joint mobility and muscle strength. (51-52) A brief period of non-weight bearing may be required to minimize undue stress on the injured syndesmotic ligaments. (25,54) An ankle stirrup does little to prevent external rotation or dorsiflexion, so a boot may be required to minimize these provocative movements. (51) Patients may begin gentle active range of motion and proprioceptive exercises as tolerated. (55) Isometric exercises should be employed in the early phase to minimize muscular atrophy. Ice, compression, elevation, and anti-inflammatory modalities or medications may provide benefit. (51,52,56)
Progression of rehab is dependent upon the severity of the injury and the patient’s response to therapy. When the patient is able to perform full weight bearing, including stairs, rehab may progress to include stretching and light resistance exercise. (51) The goal of this subacute phase is to restore pain-free function during basic activities of daily living. Stationary cycling or aquatic therapy may be useful during this stage. Proprioceptive training may reduce the recurrence of re-injury and may include an air cushion, rocker board, or BAPS board. (57-59)
Joint Mobilization
Stretching exercises should be directed at the gastroc and soleus. (55) Strengthening exercises should target the ankle stabilizers (peroneals, tibialis anterior, etc) (60) Clinicians should address hip abductor weakness to minimize excessive sway. (60) The judicious application of joint mobilization may help release restrictions and improve the range of motion. (61-65) Soft tissue techniques, including myofascial release and IASTM may be appropriate.
The final phase of rehab includes functional drills, including running, figure 8 running, jumping, plyometrics, and sports-specific drills. Dribbling, cutting, and shooting begin as tolerated and eventually progress to game speed. (51) When the patient is able to perform sports specific tasks without symptoms, they may be cleared to return to activity. (51)
The literature regarding Grade II and Grade III syndesmotic injuries is sparse, with no clear standard to guide management. (48,66-72) Diastasis of greater than 5 mm suggests ligament disruption, which precludes the ability to push off, propel, or cut. (73) Diastasis requires surgical fixation with screws to stabilize the ankle. (73)
References
1. Hopkinson WJ, St. Pierre P, Ryan JB, Wheeler JH. Syndesmosis sprains of the ankle. Foot Ankle. 1990;10:325–330.
2. Katznelson A, Lin E, Militiano J. Ruptures of the ligaments about the tibio-fibular syndesmosis. Injury. 1983;15:170–172.
3. Norkus SA, Floyd RT. The anatomy and mechanisms of syndesmotic ankle sprains. J Athl Train 2001;36(1):68–73
4. Gray H. Gray’s anatomy: the anatomical basis of medicine and surgery. 38th. New York: Churchill Livingstone; 1995.
5. Gray H. Philadelphia: Courage Books; 1999. Anatomy, Descriptive and Surgical.
6. Bartonicek J. Anatomy of the tibiofibular syndesmosis and its clinical relevance. Surg Radiol Anat. 2003;25:379–86. [PubMed]
7. Ebraheim NA, Taser F, Shafiq Q, Yeasting RA. Anatomical evaluation and clinical importance of the tibiofibular syndesmosis ligaments. Surg Radiol Anat. 2006;28:142–9.
8. Saraffian S. Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional. 2nd ed. Philadelphia: J.B. Lippincott Company; 1993.
10. Mei-Dan O, Kots E, Barchilon V, Massarwe S, Nyska M, Mann G. A dynamic ultrasound examination for the diagnosis of ankle syndesmotic injury in professional athletes. Am J Sports Med 2009;37(5):1009-16.
11. Norkus SA, R. T. Floyd RT The Anatomy and Mechanisms of Syndesmotic Ankle Sprains J Athl Train. 2001 Jan-Mar; 36(1): 68-73.
12. Norkus SA, Floyd RT. The anatomy and mechanisms of syndesmotic ankle sprains. J Athl Train 2001;36(1):68–73.
13. Houck J, Neville C, Chimenti R. The Foot and Ankle: Physical Therapy Patient Management Utilizing Current Evidence. Current Concepts of Orthopedic Physical Therapy 2012; 3: 30-31
14. Boytim MJ, Fischer DA, Neumann L. Syndesmotic ankle sprains. Am J Sports Med. 1991;19:294–8.
15. Fritschy D. An unusual ankle injury in top skiers. Am J Sports Med. 1989;17:282–5. 5–6. discussion.
16. Dattani R, Patnaik S, Kantak A, Srikanth B, Selvan TP. Injuries to the tibiofibular syndesmosis. J Bone Joint Surg Br. 2008;90:405–10.
17. Norkus SA, Floyd RT. The anatomy and mechanisms of syndesmotic ankle sprains. J Athl Train 2001;36(1):68–73
18. Dattani R, Patnaik S, Kantak A, et al. Injuries to the tibiofibular syndesmosis. J Bone Joint Surg Br 2008;90(4):405–10.
19. Boytim MJ, Fischer DA, Neumann L. Syndesmotic ankle sprains. Am J Sports Med 1991;19(3):294–8.
20. Gerber JP, Williams GN, Scoville CR, et al. Persistent disability associated with ankle sprains:
a prospective examination of an athletic population. Foot Ankle Int 1998;19(10):653–60
21. Zalavras C and Thordarson D. “Ankle Syndesmotic Injury” J Am Acad Orthop Surg June 2007; 15:330-339.
22. American Academy of Foot and Ankle Surgery. High Ankle Sprain. www.aofas.org/footcaremd/conditions/ailments-of-the-ankle/pages/high-ankle-sprain.aspx Accessed 8/14/14
23. Ivins D. Acute ankle sprain: an update. Am Fam Physician. Nov 15 2006;74(10):1714-20.
24. Van Dijk CN, Mol BW, Lim LS, Marti RK, Bossuyt PM (1996) Diagnosis of ligament rupture of the ankle joint. Physical examination, arthrography, stress radiography and sonography compared in 160 patients after inversion trauma. Acta Orthop Scand 67:566–570
25. Nussbaum ED, Hosea TM, Sieler SD, Incremona BR, Kessler DE. Prospective evaluation of syndesmotic ankle sprains without diastasis. Am J Sports Med 2001;29(1):31-5
26. Hopkinson WJ, Pierre P, Ryan JB, Wheeler JH. Syndesmosis sprains of the ankle. Foot Ankle. 1990;10(6):325-330
27. Kiter E, Bozkurt M. The crossed-leg test for examination of ankle syndesmosis injuries. Foot Ankle Int. 2005;26(2):187-188.
28. Wolf BR, Amendola A (2002) Syndesmosis injuries in the athlete. When and how to operate. Curr Opin Orthop 31:151–154
29. Cotton FJ. Dislocations and Joint-Fractures. Philadelphia, PA: WB Saunders & Co; 1911:535-588.
30. Ogilvie-Harris DJ, Reed SC. Disruption of the ankle syndesmosis: diagnosis and treatment by arthroscopic surgery. Arthroscopy. 1994;10(5):561-568.
31. Beumer A, van Hemert WL, Swierstra BA, Jasper LE, Belkoff SM (2003) A biomechanical evaluation of clinical stress tests for syndesmotic ankle instability. Foot Ankle Int 24:358–363
32. Stiell IG, Greenberg GH, McKnight RD, Wells GA. Ottawa ankle rules for radiography of acute injuries. N Z Med J. 1995;108:111
33. Dowling S, Spooner CH, Liang Y, Dryden DM, Friesen C, Klassen TP, et al. Accuracy of Ottawa Ankle Rules to exclude fractures of the ankle and midfoot in children: a meta-analysis. Acad Emerg Med. Apr 2009;16(4):277-87.
34. Plint AC, Bulloch B, Osmond MH, Stiell I, Dunlap H, Reed M. Validation of the Ottawa Ankle Rules in children with ankle injuries. Acad Emerg Med. Oct 1999;6(10):1005-9.
35. Sheyerer M, Helfet D, Wirth S, Werner C. Diagnostics in suspicion of Ankle Syndesmotic Injury. Am J Orthop. 2011; 40(4): 192-197
36. Veenema KR. Ankle sprain: primary care evaluation and rehabilitation. J Musculoske Med September 2000:563-76.
37. Clanton TO, Paul P. Syndesmotic injuries in athletes. Foot Ankle Clin N Am 2002;7:529-49
38. Wright RW, Barile RJ, Surprenant DA, Matava MJ. Ankle syndesmosis sprains in national hockey league players. Am J Sports Med. 2004;32:1941–5.
40. Uys HD, Rijke AM. Clinical association of acute lateral ankle sprain with syndesmotic involvement. Am J Sports Med 2002;30(6):816-22
41. Bencardino J, Rosenberg ZS, Delfaut E. MR imaging in sports injuries of the foot and ankle. Magn Reson Imaging Clin N Am. Feb 1999;7(1):131-49, ix
42. Chorley JN. Ankle sprain discharge instructions from the emergency department. Pediatr Emerg Care 2005;21 (8):498-501.
43. Lamb SE, Nakash RA, Withers EJ, Clark M, Marsh JL, Wilson S, et al. Clinical and cost effectiveness of mechanical support for severe ankle sprains: design of a randomized controlled trial in the emergency department. BMC Musculoskelet Disord 2005;6(1):61.
44. Beynnon BD, Renstrom PA, Haugh L, Uh BS, Barker H. A prospective, randomized clinical investigation of the treatment of first-time ankle sprains. Am J Sports Med 2006;34 (9):1401-12.
45. Bahr R, Engebretsen L. Acute ankle sprains: a functional treatment plan for injured athletes. Consultant; 1996. p. 675-88.
46. Sujitkumar P, Hadfield JM, Yates DW. Sprain or fracture? An analysis of 2000 ankle injuries. Arch Emerg Med 1986;3:101-6.
47. Veenema KR. Ankle sprain: primary care evaluation and rehabilitation. J Musculoske Med September 2000:563-76.
48. Graham A. McCollum Syndesmosis and deltoid ligament injuries in the athlete Knee Surg Sports Traumatol Arthrosc (2013) 21:1328–1337
49. Zalavras C and Thordarson D. “Ankle Syndesmotic Injury” J Am Acad Orthop Surg June 2007; 15:330-339.
50. Jones MH, Amendola A. Syndesmosis sprains of the ankle: a systematic review. Clin Orthop Relat Res. 2007;455:173–5.
51. Williams GN, Allen EJ. Rehabilitation of Syndesmotic (High) Ankle Sprains Sports Health. Nov 2010; 2(6): 460–470.
52. Chorley JN. Ankle sprain discharge instructions from the emergency department. Pediatr Emerg Care 2005;21 (8):498-501
54. Kennedy MA, Sama AE, Sigman M. Tibiofibular syndesmosis and ossification. Case report: sequelae of ankle sprain in an adolescent football player. J Emerg Med 2000;18 (2):233-40
55. Joshua C. Dubin Lateral and syndesmotic ankle sprain injuries: a narrative literature review Journ Chiro Med 2011 (10) 204-219
56. Reid DC. Sports injury assessment and rehabilitation. New York: Churchill Livingston Inc.; 1992. p. 215-68
57. McGuine TA, Keene JS. The effect of a balance training program on the risk of ankle sprains in high school athletes. Am J Sports Med 2006;34(7):1103-11.
58. Tyler TF, McHugh MP, Mirabella MR, Mullaney MJ, Nicholas SJ. Risk factors for noncontact ankle sprains in high school football players. Am J Sports Med 2006;34(3):471-5.
59. Soderberg GL, Cook TM, Rider SC, Stephenitch BL. Electromyographic activity of selected leg musculature in subjects with normal and chronically sprained ankles performing on a BAPS board. Phys Ther 1991;71(7):514-22.
60. Wilkerson GB, Pinerola JJ, Caturano RW. Invertor versus evertor peak torque and power deficiencies associated with lateral ankle ligament injury. J Orthop Sports Phys Ther 1997;26 (2):78-86
61. Reid DC. Sports injury assessment and rehabilitation. New York: Churchill Livingston Inc.; 1992. p. 215-68
62. Veenema KR. Ankle sprain: primary care evaluation and rehabilitation. J Musculoske Med September 2000:563-76.
63. Lopez-Rodriguez S, Penas CF, Alburquerque-Sendin F, Rodriguez-Blanco C, Palomeque-del-Cerro L. Immediate effects of manipulation of the talocrural joint on stabilometry and baropodometry in patients with ankle sprain. J Manipula- tive Physiol Ther 2007:186-92
64. Eisenhart AW, Gaeta TJ, Yens DP. Osteopathic manipulative treatment in the emergency department for patients with acute ankle injuries. J Am Osteopath Assoc 2003;103(9):417-21.
65. Green T, Refshauge K, Crosbie J, Adams R. A randomized control trial of a passive accessory joint mobilization on acute ankle inversion sprains. Phys Ther 2001;81(4):984-94.
66. Jones MH, Amendola A. Syndesmosis sprains of the ankle: a systematic review. Clin Orthop Relat Res. 2007;455:173–5.
67. Brown KW, Morrison WB, Schweitzer ME, Parellada JA, Nothnagel H. MRI findings associated with distal tibiofibular syndesmosis injury. AJR Am J Roentgenol. 2004;182:131–6.
68. Lynch SA. Assessment of the Injured Ankle in the Athlete. J Athl Train. 2002;37:406–12.
69. Norkus SA, Floyd RT. The anatomy and mechanisms of syndesmotic ankle sprains. J Athl Train. 2001;36:68–73.
70. Oae K, Takao M, Naito K, Uchio Y, Kono T, Ishida J, et al. Injury of the tibiofibular syndesmosis: value of MR imaging for diagnosis. Radiology. 2003;227:155–61.
71. Taser F, Shafiq Q, Ebraheim NA. Three-dimensional volume rendering of tibiofibular joint space and quantitative analysis of change in volume due to tibiofibular syndesmosis diastases. Skeletal Radiol. 2006;35:935–41.
72. Williams GN, Jones MH, Amendola A. Syndesmotic ankle sprains in athletes. Am J Sports Med. 2007;35:1197–207.
73. Taylor DC, Tenuta JJ, Uhorchak JM, Arciero RA. Aggressive surgical treatment and early return to sports in athletes with grade III syndesmosis sprains. Am J Sports Med 2007;35 (11):1833-8.








