

Diagnosis of Sacroiliac Joint Pain:
The validity of Individual Provocation Test and Composite of Tests
Chiropractic Physicians are the answer to the rising cost in back pain care. In the past several issues, I have attempted to present data that helps confirm this proposition. One of the many reasons we are the answer is our ability to use our diagnostic skills and perform a thorough examination to make an accurate diagnosis based on the information obtained. If we need advanced imaging, we can order it, but the vast majority of the time we can accurately diagnose without the need for costly tests by using clinical guidelines.
It has been my experience during my career that the sacroiliac joint (SIJ) can be a difficult diagnosis. Is the patient’s pain from the SIJ, lumbar spine or hip? The SIJ has no special distribution pattern and has no provoking or relieving movements that are unique or common to the SIJ. Therefore, we must use the best evidence available to help establish our clinical protocols to make the most accurate diagnosis. The Laslett, et a.l article on the validity of individual provocation test for the SIJ does just that by helping to establish clinical guidelines for our offices that will ensure the most accurate diagnosis. This ultimately leads to a greater understanding of the patient’s pain and effective treatment.
Advertisement
Laslett Study
Patients with buttock pain, with or without lumbar or lower extremity symptoms, were invited to participate in the Laslett study. Patients who experienced midline or symmetrical pain above the level of L5, or who had clear signs of nerve root compression (complete motor or sensory deficit) or were unwilling to participate were excluded from participating in the study. The patients were selected over a 20-month period and were not consecutive in nature. Patients were scheduled to receive an evaluation by the therapist and SIJ injection the same day with no other treatment provided. The therapist was blinded to the prior diagnostic workup of imaging or injections, and the diagnostic injection was conducted blind from the results of the SIJ provocation testing.
Patients were then evaluated by a physiotherapist with a structured examination, which included McKenzie examination of the lumbar spine, SIJ provocation test, and a hip joint assessment. The SIJ provocation tests were as follows. Distraction, thigh thrust, Gaenslen’s (right and left), compression and sacral thrust. The fluoroscopically guided contrast-enhanced SIJ orthography was performed within 30 minutes of completion of the previously mentioned examination. Pain drawings and numeric pain scales for pain intensity were acquired prior to and 30-60 minutes following diagnostic injection.
Positive SIJ Injections
48 patients satisfied the inclusion criteria and were included in the study. Of the 48 patients, 16 patients had positive SIJ injections, meaning a slow injection of solutions provoked the patient’s pain, which was followed by the introduction of a local anesthetic resulting in 80% or more relief of pain. The provocative test of the SIJ created familiar pain in those patients confirmed by diagnostic injection as having painful SIJ pathology more commonly than those with negative injections. The authors of the study then noted that there was a significant amount of false positives with the SIJ provocation test. Therefore, they analyzed the results of the SIJ provocation test when combining those provocation tests with each other and looked at the sensitivity, specificity, positive and negative predictive values. They found that if three of the six tests were positive in the examination, there was a sensitivity of 93.8% and specificity of 78.1% that the SIJ was the pain generator.
The authors then took this a step further and looked at combinations of the provocation test. It was found that the highest single positive predictive test was the distraction test, with the addition of thigh thrust, compression and sacral thrust increasing the diagnostic ability. It was found that Gaenslen’s test could be omitted from the diagnostic process because not including the test does not compromise the diagnostic confidence.
Recommended Tests
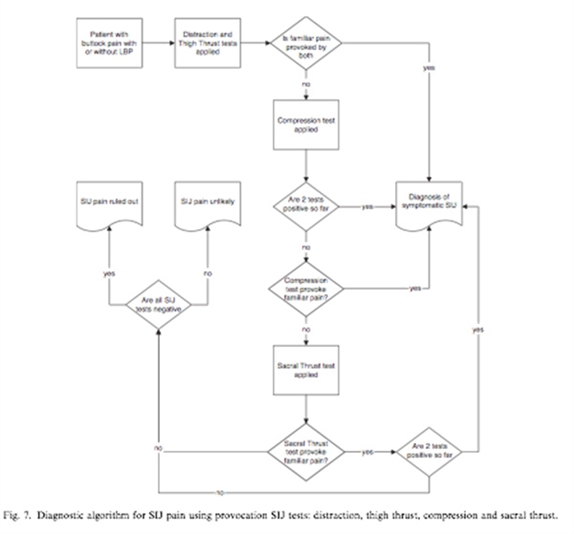
Of the 16 patients who had positive SIJ injections, only one patient out of the 16 had one positive SIJ positive test with 15 having two or more positive tests. The authors conclude that based on this information, there can be clinical rules or guidelines that may be established from the data. For instance, if all SIJ testing is negative, you can rule out SIJ pathology. If two or more provocation tests are positive for producing familiar pain, there is a high likelihood that the SIJ is the source of pain. Because thigh thrust and distraction are the most specific and sensitive, it is recommended to start with those tests first. If one is negative, then compression would be applied. If compression is positive for familiar pain then there is a high likelihood of SIJ pathology. For the complete algorithm, please refer to figure 1 (figure 7 attached).
When working with patients, I am constantly educating them on why I am performing a particular test. The test I do in the office provides a baseline for treatment and helps me understand their problem. The more we understand the patient’s complaint, the greater the likelihood that I can help them or refer them to the most appropriate provider. It is our understanding and ability to accurately identify mechanical back pain that makes us unique to the healthcare system. It is why we are the answer to the rising cost in back pain care. It is time to embrace our role, embrace evidence-based clinical guidelines and continue to provide outstanding care.
Take Home Points:
- There are no provoking or relieving movements or positions that are unique or especially common to the SIJ
- Thigh thrust and distraction are the most sensitive and specific provocative test for the SIJ
- 2 out of 4 positive SIJ provocation test increases the likelihood of the SIJ to be the source of pain for the patient
Reference
- Laslett M, et al. Diagnosis of Sacroiliac Joint Pain: Validity of individual provocation test and composite of test. Manual Therapy 2005; 10:207-18.







